1. Effect Of A Novel Anti-inflammatory Drug (dexamethasone Liposome) On Long-term Recovery Of Ischemia/reperfusion-injured Mouse Skeletal Muscle
Yu-Long LI, Dong Wang, Dongze Zhang, Fang Yuan, HuiyinTu, Jinxu Liu, Robert Muelleman. University of Nebraska, Omaha, NE
Background: Exsanguinating injury of extremity is a major cause of battlefield death. As an effective
means of arresting limb hemorrhage, tourniquet is commonly used in battle field setting. However, stopping blood flow in traumatized limb with a tourniquet,and following reperfusion also causes ischemia-reperfusion (IR) injury. During tourniquet-related IR, inflammatory cells accumulate to injured muscle to induce an inflammatory response, which results in neuronal damage and muscle function deficit and finally influences long-term recovery of muscle function.
Objectives :Our study investigated the effect of an anti-inflammatory drug (dexamethasone liposome,
Dex-lipo) on tourniquet-related skeletal muscle IR injury.
Methods: Hindlimbsof C57/BL6 mice were subjected to 3-h ischemia and 6-wks reperfusion via
placement and release of a tourniquet at the hip joint.
Results: Tourniquet-related IR led elevation of inflammatory cytokines (IL-1β and TNFα), loss of motor
nerve terminals, and skeletal muscle necrosis at the first 2-wks of IR, and hada slow recovery of motor nerve terminals and muscle contraction at 6-wks. Motornerve stimulation-induced contraction in IR gastrocnemius muscles is about 45%of normal muscle contraction. Dex-lipo (14 mg/kg) was bolus-intravenously injected at the beginning of reperfusion. Live imaging showed that Dex-lipo is
preferentially accumulated and retained at IR muscles about 2-wks. Dex-lipo not only inhibited expression of IL-1β and TNFα in IR muscle at the first 2-wks of IR, but also increased re-growing of motor nerve terminals and improved IR muscle contraction (92% of normal muscle contraction) at 6-wks of IR, compared to IR alone animals.
Conclusion: These data suggest that anti-inflammation in early stage of IR is beneficial to long-term functional recovery of neuromuscular junction and skeletal muscle from IR injury, especially novel therapeutic intervention of Dex-lipo with chemotaxis to IR-injured tissue and no Dex-associated side effects.
2. Compliance of Medications by Patients Presenting To The ED
Adam Hutnik1, Trena Burke2, Leslie Zun1, LaVonne Downey3. 1Rosalind Franklin University of Medicine and Science, North Chicago, IL; 2Mt. Sinai Hospital, Chicago, IL; 3Roosevelt University, Chicago, IL
Background:Medication noncompliance related visits to the emergency department (ED) contribute to overcrowding and a resulting compromise to patient care, and cost $8.5 billion annually. Little is known about the differences in reasons for noncompliance in psychiatric patients presenting to the ED compared to patients presenting with medical complaints.
Objectives: To identify and compare the reasons for medication noncompliance in patients presenting to the ED with psychiatric complaints in comparison to patients presenting to the ED with medical complaints.
Methods: Upon arrival to the ED, patients who were determined to be noncompliant with medications and gave consent were enrolled in the study. Upon enrollment, a short survey of questions from the validated National Health Access Survey was administered by a research fellow. The survey asked a variety of questions pertaining to healthcare accessibility and recent usage of various healthcare resources. All data was entered and analyzed by the SPSS database, version 21. This study was IRB approved.
Results: A total of 298 patients were enrolled, of which 54.4% were medical complaints and 45.6% were psychiatric complaints. Of those enrolled, 55.7% were male and 44.3% were female, 78.2% were African American, 13.4% were Hispanic, and 7.4% were Caucasian. There was no significant difference in the reasons for noncompliance in patients presenting to the ED with psychiatric complaints when compared to those presenting with medical complaints (p=0.134). The most common reason for noncompliance in both populations was an inability to afford medications, with 40.9% of respondents reporting that they were unable to afford prescription medications within the last year. The only differences that were found in these populations were that medical patients tended to take more medications on average, and psychiatric patients were more likely to visit the ED for regular care when compared to medical patients (p=0.006, p=0.005, respectively).
Conclusion: Resources need to be focused on making medication more affordable to both patient populations within this community. In addition, research needs to be done to see if these efforts are effective in improving medication compliance in both patient populations.
3. Posting of Urine Collection Instructions in Emergency Department Does Not Reduce Number of Squamous Epithelial Cells: More Comprehensive Approach Needed
Alexander Wittry, Azeemuddin Ahmed, Karisa Harland, Tyler Kempf, Sara Magill, Brett Faine. University of Iowa, Iowa City, IA
Background: The diagnosis of urinary tract infections in most patients is based on the results of a voided urinalysis and urine microscopy without the benefit of a urine culture. Contamination rates between hospitals can vary widely based on patient population, with contamination rates between 5.6% and 36.8% and a median contamination rate of 18.1%.
Objectives: To study whether the simple posting of a sign with urine collection instructions would reduce the number of squamous epithelial cells in Emergency Department urine specimens.
Methods: Urine microscopic results were abstracted for ED patients seen over six-month period. Males and all female patients with no squamous cell value, squamous value greater than 3000 or missing age were excluded. Age, gender, date of visit, weight and height was abstracted. Univariate analyses examined means and standard deviation (SD) by age, BMI, and sign presence or absence and differences examined with Student’s t-test.
Results: A total of 2382 patients met eligibility and were included in analysis. Squamous cell values did not differ statistically significantly by BMI (p=0.0601) or the presence of instruction sign (p=0.0789). In adjusted analyses, the mean squamous cell values following the instruction sign placement was lower than before the sign although not statistically significant (p=0.1165). In the analysis of all patients, controlling for the correlation within a patient, the mean squamous cell value also decreased but not statistically significant (p=0.1524).
Conclusion: The simple placement of signage describing urine collection technique reduced the number of mean squamous epithelial cells in the samples but not to a statistically significant threshold. A more comprehensive approach is needed.
4. Patient Experiences, Preferences, and Shared Decision-making In Rural Inter-hospital Transfer: A Mixed Methods Study
Terrence Wong, Nicholas Mohr, Joe Noack, Azeemuddin Ahmed, Adam Schlichting, Karisa Harland. University of Iowa - Carver College of Medicine, Iowa City, IA
Background:In the US, 1.5% of all ED visits result in inter-hospital transfer. In rural Iowa, 7-9% of all ED visits lead transfer. Despite the commonality of ED transfer, little is known about the factors that contribute to the decision to transfer a patient for a higher level of care.
Objectives: Our objective was to clarify patient attitudes and the factors that contribute to transfer decision-making.
Methods: Semi-structured interviews with adult patients transferred to a 711-bed academic medical center were conducted between May-August 2014. Three independent reviewers analyzed interview content using modified grounded theory, resolving differences through consensus and assessing for theme saturation. Standardized scenarios were used to estimate factors influencing respondents’ decision-making. Quantitative analysis was performed using standard descriptive statistics
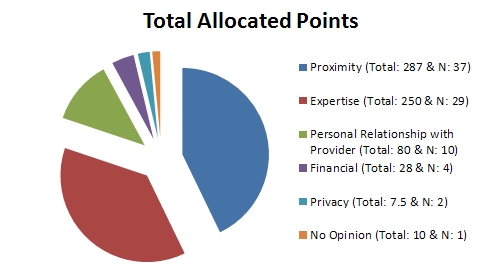
Results: Sixty-nine interviews were conducted. Only 13% of patients felt that they or family members were the primary decision maker in the transfer decision, with emergency physicians recommending the majority of transfers (59%). Participants identified five themes that influenced their decision to desire inter-hospital transfer: specialty expertise, physician relationship, proximity to home, financial factors, and personal privacy. Two scenarios were proposed to measure transfer preferences. In an intracranial hemorrhage scenario, inter-hospital transfer was desired (100-mm VAS mean 86.6, SD 2.13), and the estimated probability of intervention did not change the desire for transfer (p = 0.082). In a pneumonia scenario, participants desire for transfer was more sensitive to predicted mortality (p = 0.001), desiring transfer much more for higher predicted mortality (100-mm VAS mean 85.5 vs. 65.9, p = 0.001). Offering a telemedicine intervention decreased participants’ desire for transfer for both scenarios (p < 0.001 and p = 0.005, respectively).
Conclusion: Transfer decision-making is most commonly driven by physician recommendations, but five patient-oriented factors have been identified that patient’s value. Condition-specific factors influence patients’ likelihood to desire transfer to another facility. Telemedicine consultation was highly rated as decreasing the probability of desiring inter-hospital transfer.
Transfer Decision-maker
ER Doctor: 41
Referral Physician: 14
Self/Friend/Family: 9
Other Combination: 2
Accepting Physician: 1
Other Provider: 1
Unknown: 1
Yu-Long LI, Dong Wang, Dongze Zhang, Fang Yuan, HuiyinTu, Jinxu Liu, Robert Muelleman. University of Nebraska, Omaha, NE
Background: Exsanguinating injury of extremity is a major cause of battlefield death. As an effective
means of arresting limb hemorrhage, tourniquet is commonly used in battle field setting. However, stopping blood flow in traumatized limb with a tourniquet,and following reperfusion also causes ischemia-reperfusion (IR) injury. During tourniquet-related IR, inflammatory cells accumulate to injured muscle to induce an inflammatory response, which results in neuronal damage and muscle function deficit and finally influences long-term recovery of muscle function.
Objectives :Our study investigated the effect of an anti-inflammatory drug (dexamethasone liposome,
Dex-lipo) on tourniquet-related skeletal muscle IR injury.
Methods: Hindlimbsof C57/BL6 mice were subjected to 3-h ischemia and 6-wks reperfusion via
placement and release of a tourniquet at the hip joint.
Results: Tourniquet-related IR led elevation of inflammatory cytokines (IL-1β and TNFα), loss of motor
nerve terminals, and skeletal muscle necrosis at the first 2-wks of IR, and hada slow recovery of motor nerve terminals and muscle contraction at 6-wks. Motornerve stimulation-induced contraction in IR gastrocnemius muscles is about 45%of normal muscle contraction. Dex-lipo (14 mg/kg) was bolus-intravenously injected at the beginning of reperfusion. Live imaging showed that Dex-lipo is
preferentially accumulated and retained at IR muscles about 2-wks. Dex-lipo not only inhibited expression of IL-1β and TNFα in IR muscle at the first 2-wks of IR, but also increased re-growing of motor nerve terminals and improved IR muscle contraction (92% of normal muscle contraction) at 6-wks of IR, compared to IR alone animals.
Conclusion: These data suggest that anti-inflammation in early stage of IR is beneficial to long-term functional recovery of neuromuscular junction and skeletal muscle from IR injury, especially novel therapeutic intervention of Dex-lipo with chemotaxis to IR-injured tissue and no Dex-associated side effects.
2. Compliance of Medications by Patients Presenting To The ED
Adam Hutnik1, Trena Burke2, Leslie Zun1, LaVonne Downey3. 1Rosalind Franklin University of Medicine and Science, North Chicago, IL; 2Mt. Sinai Hospital, Chicago, IL; 3Roosevelt University, Chicago, IL
Background:Medication noncompliance related visits to the emergency department (ED) contribute to overcrowding and a resulting compromise to patient care, and cost $8.5 billion annually. Little is known about the differences in reasons for noncompliance in psychiatric patients presenting to the ED compared to patients presenting with medical complaints.
Objectives: To identify and compare the reasons for medication noncompliance in patients presenting to the ED with psychiatric complaints in comparison to patients presenting to the ED with medical complaints.
Methods: Upon arrival to the ED, patients who were determined to be noncompliant with medications and gave consent were enrolled in the study. Upon enrollment, a short survey of questions from the validated National Health Access Survey was administered by a research fellow. The survey asked a variety of questions pertaining to healthcare accessibility and recent usage of various healthcare resources. All data was entered and analyzed by the SPSS database, version 21. This study was IRB approved.
Results: A total of 298 patients were enrolled, of which 54.4% were medical complaints and 45.6% were psychiatric complaints. Of those enrolled, 55.7% were male and 44.3% were female, 78.2% were African American, 13.4% were Hispanic, and 7.4% were Caucasian. There was no significant difference in the reasons for noncompliance in patients presenting to the ED with psychiatric complaints when compared to those presenting with medical complaints (p=0.134). The most common reason for noncompliance in both populations was an inability to afford medications, with 40.9% of respondents reporting that they were unable to afford prescription medications within the last year. The only differences that were found in these populations were that medical patients tended to take more medications on average, and psychiatric patients were more likely to visit the ED for regular care when compared to medical patients (p=0.006, p=0.005, respectively).
Conclusion: Resources need to be focused on making medication more affordable to both patient populations within this community. In addition, research needs to be done to see if these efforts are effective in improving medication compliance in both patient populations.
3. Posting of Urine Collection Instructions in Emergency Department Does Not Reduce Number of Squamous Epithelial Cells: More Comprehensive Approach Needed
Alexander Wittry, Azeemuddin Ahmed, Karisa Harland, Tyler Kempf, Sara Magill, Brett Faine. University of Iowa, Iowa City, IA
Background: The diagnosis of urinary tract infections in most patients is based on the results of a voided urinalysis and urine microscopy without the benefit of a urine culture. Contamination rates between hospitals can vary widely based on patient population, with contamination rates between 5.6% and 36.8% and a median contamination rate of 18.1%.
Objectives: To study whether the simple posting of a sign with urine collection instructions would reduce the number of squamous epithelial cells in Emergency Department urine specimens.
Methods: Urine microscopic results were abstracted for ED patients seen over six-month period. Males and all female patients with no squamous cell value, squamous value greater than 3000 or missing age were excluded. Age, gender, date of visit, weight and height was abstracted. Univariate analyses examined means and standard deviation (SD) by age, BMI, and sign presence or absence and differences examined with Student’s t-test.
Results: A total of 2382 patients met eligibility and were included in analysis. Squamous cell values did not differ statistically significantly by BMI (p=0.0601) or the presence of instruction sign (p=0.0789). In adjusted analyses, the mean squamous cell values following the instruction sign placement was lower than before the sign although not statistically significant (p=0.1165). In the analysis of all patients, controlling for the correlation within a patient, the mean squamous cell value also decreased but not statistically significant (p=0.1524).
Conclusion: The simple placement of signage describing urine collection technique reduced the number of mean squamous epithelial cells in the samples but not to a statistically significant threshold. A more comprehensive approach is needed.
4. Patient Experiences, Preferences, and Shared Decision-making In Rural Inter-hospital Transfer: A Mixed Methods Study
Terrence Wong, Nicholas Mohr, Joe Noack, Azeemuddin Ahmed, Adam Schlichting, Karisa Harland. University of Iowa - Carver College of Medicine, Iowa City, IA
Background:In the US, 1.5% of all ED visits result in inter-hospital transfer. In rural Iowa, 7-9% of all ED visits lead transfer. Despite the commonality of ED transfer, little is known about the factors that contribute to the decision to transfer a patient for a higher level of care.
Objectives: Our objective was to clarify patient attitudes and the factors that contribute to transfer decision-making.
Methods: Semi-structured interviews with adult patients transferred to a 711-bed academic medical center were conducted between May-August 2014. Three independent reviewers analyzed interview content using modified grounded theory, resolving differences through consensus and assessing for theme saturation. Standardized scenarios were used to estimate factors influencing respondents’ decision-making. Quantitative analysis was performed using standard descriptive statistics
Results: Sixty-nine interviews were conducted. Only 13% of patients felt that they or family members were the primary decision maker in the transfer decision, with emergency physicians recommending the majority of transfers (59%). Participants identified five themes that influenced their decision to desire inter-hospital transfer: specialty expertise, physician relationship, proximity to home, financial factors, and personal privacy. Two scenarios were proposed to measure transfer preferences. In an intracranial hemorrhage scenario, inter-hospital transfer was desired (100-mm VAS mean 86.6, SD 2.13), and the estimated probability of intervention did not change the desire for transfer (p = 0.082). In a pneumonia scenario, participants desire for transfer was more sensitive to predicted mortality (p = 0.001), desiring transfer much more for higher predicted mortality (100-mm VAS mean 85.5 vs. 65.9, p = 0.001). Offering a telemedicine intervention decreased participants’ desire for transfer for both scenarios (p < 0.001 and p = 0.005, respectively).
Conclusion: Transfer decision-making is most commonly driven by physician recommendations, but five patient-oriented factors have been identified that patient’s value. Condition-specific factors influence patients’ likelihood to desire transfer to another facility. Telemedicine consultation was highly rated as decreasing the probability of desiring inter-hospital transfer.
Transfer Decision-maker
ER Doctor: 41
Referral Physician: 14
Self/Friend/Family: 9
Other Combination: 2
Accepting Physician: 1
Other Provider: 1
Unknown: 1
5. Predicting One-Month ED Returns in Undifferentiated Geriatric Patients: Derivation of a Clinical Decision Rule
Angela H. Lin, Christopher R. Carpenter. Washington University School of Medicine, Saint Louis, MO
Background:Geriatric patients in the emergency department (ED) are at higher risk than younger patients for avoidable short-term, post-discharge adverse outcomes such as return visits to the ED. Rapid identification of susceptible sub-populations could target preventative resources to these individuals.
Objectives: To derive a prognostic instrument that identifies community dwelling older patients in the ED who are at increased risk of ED returns within 30 days of discharge.
Methods: This was a secondary data analysis of a prospectively collected cohort of community-dwelling patients aged 65 and older presenting to one urban academic ED. Research assistants evaluated subjects in the ED using standardized assessment instruments including the Charlson Comorbidity Index (CCI) and Older American Resources and Services Activities of Daily Living (OARS-ADL). Patients were asked if they had presented to the ED during the previous 12 months. Diagnoses at ED discharge were registered from hospital records. A research assistant blinded to the baseline results obtained hospital records of ED returns at 30 after discharge. Recursive partitioning using the rpart package for R was used to identify predictor variables associated with ED returns at 30 days.
Results: Among 301 enrolled subjects, 59 (19.6%) returned to the ED within 30 days of discharge. Enrolled patients were 45.8% male and 52.5% African-American, with mean age 74.8.
We developed 5 candidate prognostic instruments consisting of ED presentation in the previous 12 months, pulmonary component to ED diagnosis, hypertension as part of ED diagnosis, CCI, OARS-ADL, and age. Patients defined as high-risk by these prognostic instruments were significantly more likely to require subsequent ED use at 30 days than the lower-risk cohort. Candidate instruments had sensitivity 12%, 42%, 46%, 17%, 56%, specificity 98%, 86%, 85%, 96%, 84%, and AUC 0.65, 0.68, 0.65, 0.68, 0.72, respectively.
Conclusion: The instruments developed in this study identify older ED patients that are at higher risk for 30-day ED returns. The predictive factors identified in these instruments do not have sufficient predictive value to recommend them for clinical use, but in conjunction with additional factors, they may be able to identify higher-risk geriatric patients in the ED.
6. Skin to Intramuscular Thigh Compartment Measurements by Ultrasound in the Pediatric Population
Myto Duong, Richard Austin, Albert Botchway. Southern Illinois University, Springfield, IL
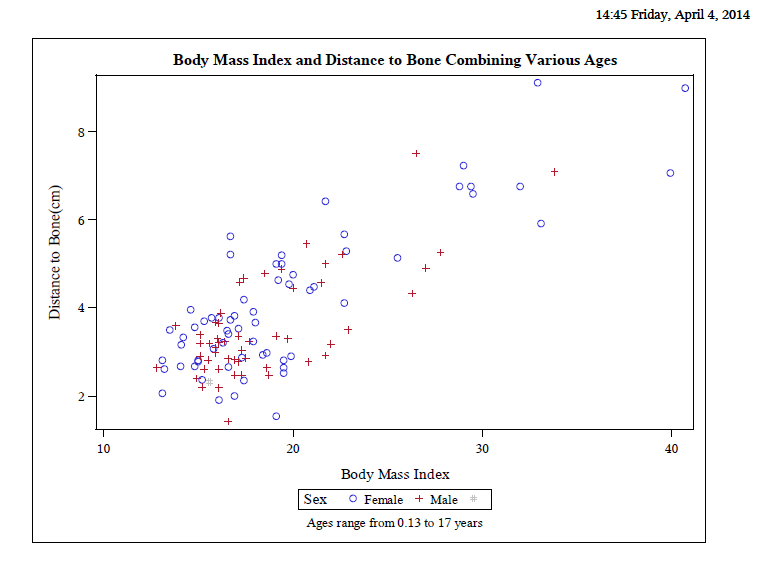
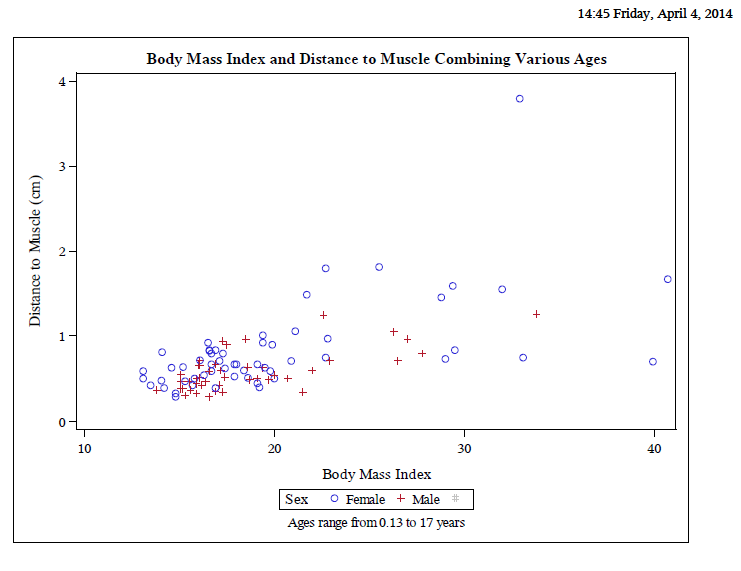
Background:Many medications and vaccines are given intramuscularly, including epinephrine in anaphylaxis, for quicker onset of action (1, 2). Blood levels of intramuscular epinephrine are therapeutic at 8 minutes versus 22 minutes when given subcutaneously (1). Pediatric obesity is a growing issue. With the increase in body habitus, problems of appropriate intramuscular medication delivery via standard needle lengths (1/2”, 5/8”, 1” and 1.5”) to these children is a great concern and potentially deadly. Stecher et al 2009 found that the epinephrine auto-injector lengths were too short to reach the muscle compartment for most pediatric patients (3). The ultimate goal of this project is to generate a graph of body mass index (BMI) versus distance to the muscle compartment to guide appropriate needle length selection for intramuscular injections.
Objectives: The objective of the study is to measure the distance from skin to thigh muscle/bone in pediatric patients of various weight and BMI.
Methods: This is a prospective, IRB approved, pilot feasibility study involving a convenience sampling of 117 pediatric patients (< 18 years of age without chronic illness which may impede normal growth and development) who present to the emergency department. Ultrasound measurements (cm) from the skin to thigh bone and muscle were obtained. Patient’s gender, age (in months), height (cm), weight (kg) and BMI were recorded. Pearson correlation coefficient was calculated.
Results: Pearson correlation coefficient for BMI to bone and muscle were 0.80 and 0.60 with p-values <0.001, respectively. The mean BMI was 19 with standard deviation of 5.3. Mean depths to bone and muscle were3.84 and 0.72 cm.
Conclusion: Although there is a linear correlation between skin to muscle and bone depth with body mass index, with more data, a non-linear curve may be more apparent. More data points are also required to further establish correlation for different age groups and gender. The graph will be useful in determining appropriate size needles required for patients of variable BMI to ensure intramuscular administration of medications or vaccines.
Angela H. Lin, Christopher R. Carpenter. Washington University School of Medicine, Saint Louis, MO
Background:Geriatric patients in the emergency department (ED) are at higher risk than younger patients for avoidable short-term, post-discharge adverse outcomes such as return visits to the ED. Rapid identification of susceptible sub-populations could target preventative resources to these individuals.
Objectives: To derive a prognostic instrument that identifies community dwelling older patients in the ED who are at increased risk of ED returns within 30 days of discharge.
Methods: This was a secondary data analysis of a prospectively collected cohort of community-dwelling patients aged 65 and older presenting to one urban academic ED. Research assistants evaluated subjects in the ED using standardized assessment instruments including the Charlson Comorbidity Index (CCI) and Older American Resources and Services Activities of Daily Living (OARS-ADL). Patients were asked if they had presented to the ED during the previous 12 months. Diagnoses at ED discharge were registered from hospital records. A research assistant blinded to the baseline results obtained hospital records of ED returns at 30 after discharge. Recursive partitioning using the rpart package for R was used to identify predictor variables associated with ED returns at 30 days.
Results: Among 301 enrolled subjects, 59 (19.6%) returned to the ED within 30 days of discharge. Enrolled patients were 45.8% male and 52.5% African-American, with mean age 74.8.
We developed 5 candidate prognostic instruments consisting of ED presentation in the previous 12 months, pulmonary component to ED diagnosis, hypertension as part of ED diagnosis, CCI, OARS-ADL, and age. Patients defined as high-risk by these prognostic instruments were significantly more likely to require subsequent ED use at 30 days than the lower-risk cohort. Candidate instruments had sensitivity 12%, 42%, 46%, 17%, 56%, specificity 98%, 86%, 85%, 96%, 84%, and AUC 0.65, 0.68, 0.65, 0.68, 0.72, respectively.
Conclusion: The instruments developed in this study identify older ED patients that are at higher risk for 30-day ED returns. The predictive factors identified in these instruments do not have sufficient predictive value to recommend them for clinical use, but in conjunction with additional factors, they may be able to identify higher-risk geriatric patients in the ED.
6. Skin to Intramuscular Thigh Compartment Measurements by Ultrasound in the Pediatric Population
Myto Duong, Richard Austin, Albert Botchway. Southern Illinois University, Springfield, IL
Background:Many medications and vaccines are given intramuscularly, including epinephrine in anaphylaxis, for quicker onset of action (1, 2). Blood levels of intramuscular epinephrine are therapeutic at 8 minutes versus 22 minutes when given subcutaneously (1). Pediatric obesity is a growing issue. With the increase in body habitus, problems of appropriate intramuscular medication delivery via standard needle lengths (1/2”, 5/8”, 1” and 1.5”) to these children is a great concern and potentially deadly. Stecher et al 2009 found that the epinephrine auto-injector lengths were too short to reach the muscle compartment for most pediatric patients (3). The ultimate goal of this project is to generate a graph of body mass index (BMI) versus distance to the muscle compartment to guide appropriate needle length selection for intramuscular injections.
Objectives: The objective of the study is to measure the distance from skin to thigh muscle/bone in pediatric patients of various weight and BMI.
Methods: This is a prospective, IRB approved, pilot feasibility study involving a convenience sampling of 117 pediatric patients (< 18 years of age without chronic illness which may impede normal growth and development) who present to the emergency department. Ultrasound measurements (cm) from the skin to thigh bone and muscle were obtained. Patient’s gender, age (in months), height (cm), weight (kg) and BMI were recorded. Pearson correlation coefficient was calculated.
Results: Pearson correlation coefficient for BMI to bone and muscle were 0.80 and 0.60 with p-values <0.001, respectively. The mean BMI was 19 with standard deviation of 5.3. Mean depths to bone and muscle were3.84 and 0.72 cm.
Conclusion: Although there is a linear correlation between skin to muscle and bone depth with body mass index, with more data, a non-linear curve may be more apparent. More data points are also required to further establish correlation for different age groups and gender. The graph will be useful in determining appropriate size needles required for patients of variable BMI to ensure intramuscular administration of medications or vaccines.
7. On the Prevalence and Clinical Significance of Coagulopathy in Chest Pain Patients
Thomas Hindsley, Charlie Inboriboon, Steven Go. University of Missouri - Kansas City, Kansas City, MO
Background:Chest pain is one of the most common and worrisome complaints in the Emergency Department. Nationwide, 5.5 million ED visits present with chest pain. A response to the impact of ED crowding on the timely evaluation chest pain has been the development of triage driven chest pain protocols. These protocols may include a variety of tests of unclear utility, one of which is coagulation studies, including PT/INR/PTT.
Objectives: The purpose of this study was to determine the incidence of unsuspected coagulapathy (INR>1.4) in patients evaluated for chest pain, determine clinically significant of these abnormalities, and to identify risk factors for unsuspected coagulopathy.
Methods: A retrospective cross sectional chart review was conducted on 1500 sequential adult presentations for chest pain at an urban academic emergency department. The charts were electronically and manually reviewed to collect patient age, gender, race, past medical history, anticoagulation therapy, social history, laboratory values, disposition, length of stay, heparinization,, use of blood products, reversal of anticoagulation, and inpatient mortality. Patients with multiple ED visits or traumatic chest pain were excluded, and a total of 1192 patients were included in the statistic analysis.
Results: 29 patients (2.4%) presenting with chest pain were coagulopathic without any identifiable risk factor. There was a statistically significant association of unsuspected coagulopathy with admission rates (97% vs 70% for controls) and for inpatient mortality rates (6.9% vs 0.6%). Given the small sample size of patients with unsuspected coagulapathy, no significant difference in risk factors was found between controls and unsuspected coagulopaths.
Conclusion: The number of chest pain patients who were found to have an unsuspected coagulopathy was low, and comparable to prior population studies. Chest pain patients with unsuspected coagulapathy were more likely to be admitted and more likely to die in the hospital. There is a need for further higher powered studies to determine what factors may be predictive of unsuspected coagulopathies.
8. Bedside Ultrasonography for The Detection Of Apnea During Simulated Procedural Sedation
Jennifer Marshalla, Tyler Fulks, Maddelynn Hawkins, BreeAnna Groves, Erik Curry, Richard Austin, Jonathan dela Cruz. Southern Illinois University School of Medicine, Springfield, IL
Background:Previous studies have shown that end-tidal carbon dioxide (ETCO2) monitoring is the earliest indicator and gold standard for the detection of apnea during procedural sedation. When ETCO2 is not available, current standard of practice calls for pulse-oximetry and direct physical assessment for apnea. This approach can lead to delayed intervention as measurable hypoxia commonly occurs sometime after the onset of apnea. Thoracic ultrasound has been proven to be both sensitive and specific for detecting lung and diaphragmatic movement and could possibly be used as an adjunct for assessing apnea.
Objectives: To determine the utility of ultrasound in detecting apnea during procedural sedation using a simulated patient encounter.
Methods: A retrospective observational study was used in conjunction with a senior resident milestone evaluation for procedural sedation. Five PGY-3 EM residents were assessed in their ability to manage the airway of a simulated procedural sedation encounter. A 25 year old male standardized patient was used to simulate episodes of apnea (defined as breathing 6 times per minute). Residents actions of detecting and intervening on these episodes were recorded both with and without the use of thoracic ultrasound. Residents were prompted with hypoxic alerts on a simulated monitor after 2 minutes of simulated apnea. Time to detection and intervention were then compared with respect to ultrasound use.
Results: Each resident encountered 2-4 episodes of simulated apnea both with and without the use of ultrasound. We identified that, on average, residents detected apnea without the use of ultrasound in 42.62 seconds and intervened on apneic episodes 9.02 seconds later. With the use of ultrasound, on average, residents detected apnea in 42.98 seconds and intervened on apneic episodes 2.0 seconds later.
Conclusion: Our data showed the detection of apnea on a standardized patient by residents was similar with and without the use of ultrasound. However, residents intervened during episodes of apnea 7 seconds faster with ultrasound, demonstrating an increased confidence in clinical detection of apnea. Further research is needed to determine the clinical significance of this decreased time to intervention and to determine if these results are generalizable to non-simulated patient encounters.
9. Characterizing Resident Physician Utilization of IVC Ultrasonography Versus Invasive Central Venous Pressure Monitoring In Guiding Fluid Resuscitation In Severe Sepsis And Septic Shock
Mohammad Subeh. University of Chicago, Chicago, IL
Background:In patients with severe sepsis or septic shock, goal-directed fluid resuscitation during the first 6 hours of care is recommended. Techniques for guiding fluid resuscitation include invasive central venous pressure (CVP) monitoring and ultrasound (US) measurement of inferior vena cava (IVC) respiratory variation. CVP monitoring is often not performed for these patients in emergency departments (EDs) for a variety of reasons. IVC US is also under-utilized, primarily because resident training in this technique has been variable across institutions nationally.
Objectives: To quantify resident physician utilization of IVC US versus CVP monitoring to guide fluid therapy in severe sepsis and septic shock prior to implementation of a formal curriculum in bedside IVC US.
Methods: This is a retrospective chart review of all patients presenting with severe sepsis or septic shock to a single ED from July to December 2012. Severe sepsis was defined as sepsis plus sepsis-induced organ dysfunction, elevated lactate, or markedly abnormal vital signs. Septic shock was defined as sepsis plus systolic BP <90 despite a 30 cc/kg saline challenge.
Results: Fifty-seven (57) patients presented with severe sepsis or septic shock during the 6-month period. The mean age was 62.4 years (range 25-91 years). Thirty-one (31) patients met the criteria for severe sepsis and 26 for septic shock. During the first 6 hours of ED care, the median volume of saline infused was 2.0 L (range 0-7 L). CVP was monitored in none of the patients with severe sepsis and in 7 of 26 patients (26.9%) with septic shock. IVC US was performed in 1 of 31 patients (3.2%) with severe sepsis and in none of the patients in septic shock. Overall mortality was 37% (severe sepsis 29%, septic shock 46%).
Conclusion: In this urban ED, CVP monitoring was uncommonly used in patients presenting with severe sepsis or septic shock. Monitoring IVC respiratory variation by US is a useful alternative technique to guide fluid resuscitation in these patients, but was used even less (in only 1 of 57 patients). The under-utilization of these techniques was associated with inadequate fluid therapy and a high mortality rate. Implementation of IVC US training for resident physicians and formal integration within ED sepsis management protocols can improve outcomes for these critically ill patients.
10. Emergency Department Central Line Associated Blood Stream Infections (CLABSI) Incidence in the Era of High Prevention
Daniel L. Theodoro1, Margaret A. Olsen1, David K. Warren1, Kathleen M. McMullen2, Phillip Asaro1, Adam Henderson1, Michael Tozier1, Victoria Fraser1. 1Washington University School of Medicine in St. Louis, St. Louis, MO; 2Barnes Jewish Hospital, St. Louis, MO
Background: The incidence of central line associated blood stream infections (CLABSI) among central venous catheters (CVC) inserted in the Emergency Department (ED) is not well tracked or reported.
Objectives:Our goal was to determine the rate of ED CLABSI during an era of increased focus on CLABSI prevention practices.
Methods: This was a prospective observational study over a 28-month time period from March 2008 to June 2010 at a single academic tertiary care center. After month 13 a CVC insertion bundle was introduced hospital-wide by infection prevention to standardize insertion practices and prevent CLABSIs. Using the electronic ED health record, a standardized CVC procedure note was created to identify CVC insertions taking place in the ED. Trained abstractors reviewed ED records of patients with CVC to determine ED CVC catheter-days. Blood culture results up to 2 days after ED CVC removal were obtained from a hospital informatics database and an infection prevention specialist identified CLABSIs originating in the ED using National Hospital Safety Network definitions. ED CLABSI rates were compared to institutional CLABSI rates collected by infection prevention for routine surveillance. Administrative data, also obtained from the hospital informatics database were used to determine the sensitivity of billing data in identifying CVCs inserted in the ED. Results were analyzed using proportions and 95% confidence intervals.
Results: The ED CLABSI rate was 2.0/1,000 catheter days (95% CI, 1.0 to 3.8). The concurrent institutional composite intensive care unit (ICU) CLABSI rate was 2.3/1,000 catheter days (95% CI 1.9-2.7). Eight CLABSIs occurred before the introduction of a CVC prevention bundle and 1 occurred after. Clinical Procedural Terminology (CPT) codes detected 74% (95% CI 71-77%) of CVCs inserted in the ED and International Classification of Diseases, 9th edition (ICD-9) procedure codes detected 57% (95% CI, 53-59%); together CPT or ICD-9 codes detected 88% (95% CI, 86-90%) of ED CVC insertions.
Conclusion: Composite ED CLABSI rates were in the range of those reported by the ICUs. Combining hospital and physician billing information improves the sensitivity of administrative data. Further research dedicated to surveying ED CLABSI rates are necessary to determine the impact of CLABSI prevention practices in the ED.
11. Early Goal-Directed Therapy Compliance in Patients Transferred with Severe Sepsis or Septic Shock to a Large Academic Hospital
Joseph Noack, Nicholas Mohr, Brett Faine, Terrence Wong, Azeemuddin Ahmed. University of Iowa, Iowa City, IA
Background:Sepsis is a life-threatening condition that relies heavily on early recognition and treatment. Early goal-directed therapy (EGDT) has decreased the mortality rate of sepsis nearly 25% in the last two decades. Many patients in rural areas who present with sepsis are transferred to a larger hospital to receive specialized care. The question of whether inter-transfer interrupts the delivery of early goal-directed therapy has not yet been answered.
Objectives: The aim of the study was to identify if inter-hospital transfer from rural institutions to larger institutions results in delays in time sensitive care for patients with severe sepsis or septic shock.
Methods: A retrospective cohort analysis was conducted on patients who presented to the University of Iowa Hospitals and Clinics (UIHC) Emergency Department (ED) with severe sepsis or septic shock following transfer from a regional hospital from 2009-2014. Patients who presented directly to the UIHC ED served as controls. Comparisons of treatment times were analyzed with chi-square and two-tailed t-test calculations to identify differences in care between the two cohorts.
Results: Data was collected from 38 transfer patients and 135 control patients. Patients with an abdominal (p=0.010) or necrotizing fasciitis (p=0.003) source of sepsis were more likely to be transferred, while patients with pneumonia were less likely to be transferred (p=0.028). The transfer patients were more likely to get surgery while at UIHC (p<0.001), but only 55.3% of the transfer patients needed surgery. Transfer patients spent more time in the ED before being admitted to the inpatient unit (10.36±6.0 hours vs. 4.18±1.95 hours, p=0.001). While in the ED, transfer patients were more likely to receive adequate fluid resuscitation (p=0.031), receive vasopressors (p=0.03), and have placement of a central venous catheter (p=0.008). The time to first antibiotic in the study group was 3.23±3.28 hours compared to 2.05±1.42 hours in the control group (p=0.042).
Conclusion: Inter-hospital transfer leads to significant treatment delays in patients with severe sepsis and septic shock. Future studies should evaluate interventions to increase the early recognition and treatment of sepsis patients presenting to rural hospitals.
12. The Recognition of Hospice Eligible Patients In The Emergency Department: A Missed Opportunity
Melissa Bacci, Karisa Harland, Adam Schlichting, Andrew Nugent. The University of Iowa, Iowa City, IA
Background: Integrating palliative medicine and hospice services into emergency medicine is essential to providing optimal patient care, yet it remains unknown how well emergency department (ED) clinicians recognize hospice eligible patients. Early recognition of these patients in the ED could lead to more timely access to palliative care (PC) that could substantially improve their quality of life.
Objectives: To identify hospice eligible ED patients based on current guidelines and to determine whether they were identified and treated as such by the ED treating staff.
Methods: A retrospective chart review was completed for all ED visits of adults 65 years of age and older at a large academic medical center from September-November 2013. Physician and social work notes, including those from the ED visit, were evaluated for hospice eligibility using criteria from the National Hospice and Palliative Care Organization and Medicare guidelines. Hospice eligibility was evaluated, as no objective measure to assess PC eligibility exists. To examine recognition of hospice eligibility, the occurrence of PC discussions in the ED, PC consults initiated from the ED, and hospice referrals for eligible patients were recorded. Patients already enrolled in hospice were excluded.
Results: Out of 1884 ED visits reviewed, 237 visits (12.5%) were by patients that met hospice eligibility criteria. Almost half of these visits (n=114, 48%) were by patients who had been seen in the ED in the previous 12 months, and of those with prior visits, 50% (n=58) had multiple visits. PC discussions were documented in 7.6% (n=18) of visits. Among those with PC discussions, over half (10 of 18) did not receive a PC consult or hospice referral from the ED.
Conclusion:The majority of hospice eligible ED patients 65 years of age and older went unrecognized in the ED and had no documented PC discussion. Even among those with a discussion, many received no consult or referral. As a result, only a fraction of patients who may have benefitted from PC were offered the opportunity to utilize it. Our findings illustrate the importance of educating ED staff, as well as creating automated electronic tools that alert staff to potential hospice eligible patients. Improving the recognition of these patients may lead to more timely and appropriate use of PC services that in turn, provide the highest quality of care to these patients and their families.
13. MINI Kid Study: Emergency Department Screening for Psychiatric Illness in Pediatric Patients
Jacqueline L. Nguyen1, La Vonne A. Downey2, Trena M. Burke1, Leslie S. Zun1. 1Chicago Medical School, North Chicago, IL; 2Roosevelt University, Chicago, IL
Background:Pediatric mental health disorders currently afflict 21-23% of children and adolescents in the US. Adolescents frequently visit the Emergency Department (ED) because many do not have access to a primary care provider. However, up to 98% of mental health problems in pediatric patients go undetected by ED physicians.
Objectives: To identify unsuspected psychiatric illness in adolescent patients who present to the ED with non-psychiatric complaints using a validated survey tool: the MINI International Neuropsychiatric Interview for Children and Adolescents (M.I.N.I. KID) and to evaluate the effectiveness of referrals administered.
Methods: After patients assented and parents/guardians consented, all patients (ages 12-17) with non-psychiatric complaints were enrolled and interviewed using the MINI Kid. ED physicians were notified of patients who tested positive for mental illness and patients were referred to a mental health worker for evaluation. After discharge, patients were contacted to follow-up regarding their psychiatric treatment. Data was analyzed using SPSS version 21. This study was IRB approved.
Results: A total of 175 patients were enrolled, the majority consisted of 56.6% African American and 42.3% Hispanic. Using the MINI Kid, 44.6% (78) of patients tested positive for 1 or more modules. Of patients who tested positive for mental disorders, 35.9% (28) tested positive for 1 module, 16.7% (13) tested positive for 2 modules and 47.4% (37) tested positive for 3 or more modules.
The most common modules are: Major Depressive Episode Current - 6.3% (11), ADHD Combined - 5.7% (10), Agoraphobia without History of Panic Disorder - 4.6% (8), and Oppositional Defiant Disorder - 4.0% (7). Of those who tested positive, only 10.3% (6) of patients used any services; but the majority of patients who contacted resources, found the referrals helpful.
Conclusion: The MINI Kid Interview is a beneficial tool to screen ED pediatric patients for undiagnosed mental disorders. However, ED patients exhibit low compliance to utilize referrals to receive proper psychiatric aid. Further studies should be conducted to improve patient adherence to mental health referrals and follow-up. Early mental health screening for psychiatric illness is vital to identify mental disorders in patients and improve overall long-term health outcome.
14. Assessment and Referral for Treatment of Patients at Risk for Suicide in the Emergency Department
Paul Vithayathil1, Trena Burke2, LaVonne Downey3, Leslie Zun1. 1Chicago Medical School at Rosalind Franklin University, North Chicago, IL; 2Mt. Sinai Hospital Emergency Department, Chicago, IL; 3Roosevelt University, Chicago, IL
Background: ED visits for suicide attempts have increased by 47% in the last 10 years. 40% of completed suicides among individuals over 16 years were seen in the ED one year before. Screening in ED could potentially capture these patients.
Objectives:Identify patients with non-suicide related illness presenting to the ED who might be at risk for suicide and refer them to appropriate services.
Methods: We sought to enroll 300 patients by convenience sampling in the ED of a Midwest urban level 1 trauma center. Subjects were consented and administered the Columbia-Suicide Severity Rating Scale (C-SSRS) to determine if it identifies patients at risk for suicide. The C-SSRS has 6 questions, has been validated for use in the ED, and administration takes less than 5 minutes. Inclusion criteria were all consenting English speaking medically stable patients. Exclusion criteria were patients who are not medically stable, do not give consent, and are non-English speaking. Data was analyzed by SPSS (ver. 14, IBM).This was an IRB approved study.
Results: 300 patients were enrolled by convenience sampling. The sample demographics were as follows: 56.7% (170) female, 75.7% (227) African American, Average Age: 37.03 (std. dev. 15.820)
The C-SSRS was effective in identifying patients at risk for suicide. 19% (57) of patients screened positive. Of the positives, 70% (40) had past suicidal behavior, and 14% (8) had current thought, intent, plan, and method. Psychiatric complaints represented 100% (5) of cases with positive current suicidal intent and method in the 18-21 (2) and 45-54 (3) age range (F=1.952, p= 0.011). Current suicidal ideation was higher in females than males (3.6% (6) vs. 1.6% (2) of all cases).
Conclusion: Consistent with previous studies showing females and younger patients as higher risk. The C-SSRS identified patients with psychiatric disease with highest risk of current suicidal ideation. We recommend screening psychiatric patients for current suicidal ideation and intent. Musculoskeletal complaints were correlated with past suicidal behavior in young patients and respiratory complaints were associated with elderly patients. Because past suicidal behavior is a major risk factor for future attempts, we recommend screening younger patients with musculoskeletal complaints and elderly patients with chronic respiratory issues.
15. Reasons for Psychiatric Readmissions to the Emergency Department
Loryn Wilson1, Leslie Zun1, Trena Burke1, LaVonne Downey2. 1Mt. Sinai Hospital - Rosalind Franklin University, Chicago, IL; 2Roosevelt University, Chicago, IL
Background:Emergency Departments (EDs) have become increasingly overcrowded and this has the potential to impact quality and accessibility of care. Frequent users of the ED contribute to the problem of overcrowding and are more likely to have psychiatric problems. In addition, ED visits due to mental health problems have increased in recent years.
Objectives: To determine the reasons for return ED visits of psychiatric patients.
Methods: This is a retrospective chart review of a random sample of 350 psychiatric patients who presented to the ED and had a return visit within 90 days. This study was conducted at a 432 bed, urban, level I adult and pediatric trauma center with 50,000 ED visits per year. The inclusion criterion was all psychiatric patients who presented to the ED since January 2010 and had a least one return visit within 90 days. The exclusion criterion was patients who presented with non-psychiatric complaints. SPSS version 14 was used, and the study was IRB approved.
Results: The most common psychiatric diagnoses for each of three visits within 90 days were depression, schizophrenia, schizoaffective disorder, bipolar disorder, and psychosis. The most common reasons for the second visit were 1. Psychiatric (61.9%), 2.Musculoskeletal (9.2%), 3.Cardiovascular (5.7%), 4. Neurological (4.3%), and 5. Dermatological (3.2%) complaints while the most common reasons for the third visit were 1. Psychiatric (55.4%), 2.Musculoskeletal (7.0%), 3.Drug/alcohol abuse (7.0%), 4.Neurological (6.1%), and 5. Dermatological (4.6%) complaints. ANOVA analysis showed that there was a significant difference in the reasons for the second and third visit (p = 0.001). The admission rate for each visit was 51.4% for the first, 44.1% for the second, and 35.5% for the third.
Conclusion: Psychiatric patients are not returning to the ED repeatedly for the same complaints or for only psychiatric complaints. Musculoskeletal complaints were the most common reason for return (after psychiatric complaints), and depression was the most common psychiatric complaint observed.
16. Utilization of the ED for Violence Prevention Referrals
Nicholas Leader1, Leslie Zun1, LaVonne Downey2, Trena Burke3. 1Chicago Medical School, Rosalind Franklin University of Medicine and Science, North Chicago, IL; 2Roosevelt University, Chicago, IL; 3Department of Emergency Medicine, Mount Sinai Hospital, Chicago, IL
Background:The rate of violence in the inner city population is at epidemic proportions. Homicide is the second leading cause of death for youth in the US between the ages of 15-24, with over 82% of these cases being attributable to firearms. Many of these victims present to the Emergency Department for treatment, which previous studies have found to be an effective location for patient intervention.
Objectives: The purpose of this study is to determine the effectiveness of an ED-based violence prevention referral.
Methods: A convenience sample of medically stable patients aged 16-24 years old presenting to the emergency department as victims of interpersonal violence were eligible. The study was conducted at an urban, teaching level 1 trauma center. After patient consent was obtained, a violence prevention brochure containing available referral sources was provided. Participants were contacted after discharge by their preferred method: phone call, text message, or email. Data was analyzed using SPSS version 14. This study was approved by the IRB.
Results: Two hundred thirty-six victims of interpersonal violence that met the criteria were enrolled in the study. The average age was 20.5 and 81.8% were male. Of those enrolled, 71.6% were African American and 25.8% were Hispanic. Gunshot wounds accounted for 59% (n=141) of the diagnoses.
Phone call was the preferred method of contact for 86.4% of the patients, followed by text message (7.2%) and email (6.4%). Nearly half (49.2%, n=116) of the first follow up attempts were successful, while 14% (n=33) of the second attempts were achieved. Overall, only 10.6% (n=25) of the patients enrolled in the study utilized the referral brochure. The top three resources that were contacted include: anti-violence victim hotline, job training, and financial service.
Conclusion: Providing a brochure with referrals to victims of violence is not a very effective ED intervention strategy, although majority (76%, n=19) that did contact the resources found them to be helpful. Alternative forms of intervention should be tested, considering that victims of violence have an alarming rate of recidivism in conjunction with more aggressive retaliatory attitudes.
17. Changes in Emergency Department Volumes in Winter 2014
Hans House, Ben Oglivie. University of Iowa - Carver College of Medicine, Iowa City, IA
Background:Emergency department (ED) visits can be affected by weather and changes in access. In 2014, the Affordable Care Act was fully implemented. The American College of Emergency Physicians (ACEP) conducted a poll in April 2014 asking members about changes in ED patient volume, number of Medicaid patients, and acuity of visits seen in the first three months of 2014.
Objectives: The aim of this study is to examine for regional differences in emergency department visits and payer mix for the first quarter of 2014 (January - April).
Methods: We obtained the raw data of the ACEP poll. We analyzed the data collected from all 50 states focusing on emergency department visits and payer mix. We then categorized the 48 contiguous United States regionally by using the National Climatic Data Center (NCDC) nine climatically consistent regions, which was assembled to put climate anomalies into a historical perspective.
Results: The poll was conducted from April 4 - 14, 2014, with 1845 physicians polled and a 8% response rate. Collectively, 46% of respondents report an increase in ED volume, 27% report no change, and 23% report a decrease in volume. A plurality report an increase in volume in every region except the Upper Midwest (IA, MI, MN, WI). There, 22% report an increase, 30% report no change, and 42% report a drop in ED census. The largest increases in patient volume were seen in the West region (66%). Collectively, most ED’s report more Medicaid patients and fewer privately insured patients. There was no difference in changes to payer mix by climate region, but ACEP’s own analysis found that states that expanded Medicaid saw an increase in Medicaid patients.
Conclusion: There were significant differences in reported volume changes regionally. Since the implementation of the Affordable Care Act (ACA), most ED’s have seen an increase in the number of patients, especially in states that expanded Medicaid coverage. But the Upper Midwest, on the average, saw a drop in the total number of patients. This may be due to the abnormally cold winter experienced this year. However, the Northeast experienced a very cold winter as well and 41% experienced an increase in census.
18. Comparison of Interpreters in the Emergency Department
Jason E. Smith1, Trena M. Burke1, LaVonne Downey2, Leslie S. Zun1. 1Chicago Medical School, North Chicago, IL; 2Roosevelt University, Chicago, IL
Background:Communication barriers between emergency department (ED) staff and limited English proficiency (LEP) patients have fundamental impacts on patient care and satisfaction. As LEP patients are a significant and growing minority of those seen in the ED, continual evaluation of different interpretation methods is needed.
Objectives: To determine the effects of three different interpretation modalities with regards to patient satisfaction and understanding, health care provider satisfaction, length of stay and cost of care in the ED.
Methods: This study occurred at an inner city level one trauma center with 60,000 ED visits per year. Medically stable Spanish speaking patients, 18 years and older, presenting to the ED were enrolled. After consent, patients received one of three different interpreter services: a hospital provided interpreter (LIVE), physicians/nurses that spoke Spanish, or a videoconferencing technology (IVIN).
Patient satisfaction and understanding, and health care provider satisfaction were assessed with a brief survey. Statistical analysis was performed with SPSS (ver. 14, IBM). ANOVA tests were used to determine statistical significance. A p value < 0.05 was considered statistically significant.
This study was IRB approved.
Results: A total of 82 patients were enrolled. Of those, 99% were Hispanic and 52% were female. Average age was 49 (SD 17.4). 43 patients used hospital provided interpreters, 20 patients had a Spanish speaking physician or nurse and 19 used the videoconferencing technology, IVIN.
There were no significant differences between reported patient satisfaction, patient ease of understanding, or health care provider satisfaction between groups.
Additionally, there were no significant differences in length of stay or total charges between groups. Finally, there was no association between type of interpreter service used and assessed patient acuity.
Conclusion: Providing interpreter services to Spanish speaking LEP patients resulted in high degrees of patient satisfaction and understanding, regardless of modality.
Additionally, this study demonstrated that an on-demand videoconferencing interpreter system could be part of the solution to providing sufficient interpreter services to LEP patients.
19. A Collaborative Approach to Reducing Emergency Department Overcrowding
Erin Willard, Seamus Murphy, Elizabeth Carlton, Bradley E. Barth. University of Kansas, Kansas City, KS
Background: Emergency department (ED) overcrowding is a national issue.
Objectives:After previously reporting on the effectiveness of using an ED Flow Coordinator to improve patient throughput, we developed a plan known as the Full Capacity Protocol (FCP). The FCP is a pre-determined response that calls for leaders from various departments to descend on the ED and collaborate to identify and remove barriers to patient flow. The goal is to create a system in which patient admission is a safe, fluid process that involves equal ED pushing and hospital pulling to achieve optimal outcomes. This study examined the effectiveness of the FCP in achieving that goal.
Methods: This retrospective observational study examined various hospital and ED metrics before and after implementation of the FCP. We compared the first six months the protocol was in use to the corresponding six months from the year prior to implementation. Two analyses were performed: one that examined cumulative data during these time periods and one that compared days on FCP in 2014 to similar days in 2013 (Prior to FCP). Statistical significance was measured using two-sided t-tests. Binomial proportion confidence intervals were calculated using the Wilson score interval method.
Results: The cumulative analysis showed a 7.4% increase in ED encounters (p<0.001) and an 11.9% increase in ED admissions (p<0.001) compared to the corresponding time period in 2013. The ED also saw a 10.2% decrease in total LWBS that was not statistically significant (p=0.29), an increase in LOS of 34 minutes (p<0.001), and a 92% decrease in ambulance diversion (111 fewer hours). In the second analysis, the 27 days on FCP were compared to similar days (matched by volume and acuity) from the previous year. Similar the LOS was higher for FCP days (p<0.001). The LWBS rate subsequent to FCP activation was less (p<0.05) than that of similar days from the previous year. On days the FCP was activated, the rate of hospital admissions was increased (p<0.05).
Conclusion: A FCP is effective in reducing LWBS, ambulance diversion, and accommodating increased hospital admission rates while also allowing for a significant increase in ED volume. This indicates that a multidisciplinary approach can generate substantial improvements in a hospital’s ability to address ED overcrowding and patient throughput.
Thomas Hindsley, Charlie Inboriboon, Steven Go. University of Missouri - Kansas City, Kansas City, MO
Background:Chest pain is one of the most common and worrisome complaints in the Emergency Department. Nationwide, 5.5 million ED visits present with chest pain. A response to the impact of ED crowding on the timely evaluation chest pain has been the development of triage driven chest pain protocols. These protocols may include a variety of tests of unclear utility, one of which is coagulation studies, including PT/INR/PTT.
Objectives: The purpose of this study was to determine the incidence of unsuspected coagulapathy (INR>1.4) in patients evaluated for chest pain, determine clinically significant of these abnormalities, and to identify risk factors for unsuspected coagulopathy.
Methods: A retrospective cross sectional chart review was conducted on 1500 sequential adult presentations for chest pain at an urban academic emergency department. The charts were electronically and manually reviewed to collect patient age, gender, race, past medical history, anticoagulation therapy, social history, laboratory values, disposition, length of stay, heparinization,, use of blood products, reversal of anticoagulation, and inpatient mortality. Patients with multiple ED visits or traumatic chest pain were excluded, and a total of 1192 patients were included in the statistic analysis.
Results: 29 patients (2.4%) presenting with chest pain were coagulopathic without any identifiable risk factor. There was a statistically significant association of unsuspected coagulopathy with admission rates (97% vs 70% for controls) and for inpatient mortality rates (6.9% vs 0.6%). Given the small sample size of patients with unsuspected coagulapathy, no significant difference in risk factors was found between controls and unsuspected coagulopaths.
Conclusion: The number of chest pain patients who were found to have an unsuspected coagulopathy was low, and comparable to prior population studies. Chest pain patients with unsuspected coagulapathy were more likely to be admitted and more likely to die in the hospital. There is a need for further higher powered studies to determine what factors may be predictive of unsuspected coagulopathies.
8. Bedside Ultrasonography for The Detection Of Apnea During Simulated Procedural Sedation
Jennifer Marshalla, Tyler Fulks, Maddelynn Hawkins, BreeAnna Groves, Erik Curry, Richard Austin, Jonathan dela Cruz. Southern Illinois University School of Medicine, Springfield, IL
Background:Previous studies have shown that end-tidal carbon dioxide (ETCO2) monitoring is the earliest indicator and gold standard for the detection of apnea during procedural sedation. When ETCO2 is not available, current standard of practice calls for pulse-oximetry and direct physical assessment for apnea. This approach can lead to delayed intervention as measurable hypoxia commonly occurs sometime after the onset of apnea. Thoracic ultrasound has been proven to be both sensitive and specific for detecting lung and diaphragmatic movement and could possibly be used as an adjunct for assessing apnea.
Objectives: To determine the utility of ultrasound in detecting apnea during procedural sedation using a simulated patient encounter.
Methods: A retrospective observational study was used in conjunction with a senior resident milestone evaluation for procedural sedation. Five PGY-3 EM residents were assessed in their ability to manage the airway of a simulated procedural sedation encounter. A 25 year old male standardized patient was used to simulate episodes of apnea (defined as breathing 6 times per minute). Residents actions of detecting and intervening on these episodes were recorded both with and without the use of thoracic ultrasound. Residents were prompted with hypoxic alerts on a simulated monitor after 2 minutes of simulated apnea. Time to detection and intervention were then compared with respect to ultrasound use.
Results: Each resident encountered 2-4 episodes of simulated apnea both with and without the use of ultrasound. We identified that, on average, residents detected apnea without the use of ultrasound in 42.62 seconds and intervened on apneic episodes 9.02 seconds later. With the use of ultrasound, on average, residents detected apnea in 42.98 seconds and intervened on apneic episodes 2.0 seconds later.
Conclusion: Our data showed the detection of apnea on a standardized patient by residents was similar with and without the use of ultrasound. However, residents intervened during episodes of apnea 7 seconds faster with ultrasound, demonstrating an increased confidence in clinical detection of apnea. Further research is needed to determine the clinical significance of this decreased time to intervention and to determine if these results are generalizable to non-simulated patient encounters.
9. Characterizing Resident Physician Utilization of IVC Ultrasonography Versus Invasive Central Venous Pressure Monitoring In Guiding Fluid Resuscitation In Severe Sepsis And Septic Shock
Mohammad Subeh. University of Chicago, Chicago, IL
Background:In patients with severe sepsis or septic shock, goal-directed fluid resuscitation during the first 6 hours of care is recommended. Techniques for guiding fluid resuscitation include invasive central venous pressure (CVP) monitoring and ultrasound (US) measurement of inferior vena cava (IVC) respiratory variation. CVP monitoring is often not performed for these patients in emergency departments (EDs) for a variety of reasons. IVC US is also under-utilized, primarily because resident training in this technique has been variable across institutions nationally.
Objectives: To quantify resident physician utilization of IVC US versus CVP monitoring to guide fluid therapy in severe sepsis and septic shock prior to implementation of a formal curriculum in bedside IVC US.
Methods: This is a retrospective chart review of all patients presenting with severe sepsis or septic shock to a single ED from July to December 2012. Severe sepsis was defined as sepsis plus sepsis-induced organ dysfunction, elevated lactate, or markedly abnormal vital signs. Septic shock was defined as sepsis plus systolic BP <90 despite a 30 cc/kg saline challenge.
Results: Fifty-seven (57) patients presented with severe sepsis or septic shock during the 6-month period. The mean age was 62.4 years (range 25-91 years). Thirty-one (31) patients met the criteria for severe sepsis and 26 for septic shock. During the first 6 hours of ED care, the median volume of saline infused was 2.0 L (range 0-7 L). CVP was monitored in none of the patients with severe sepsis and in 7 of 26 patients (26.9%) with septic shock. IVC US was performed in 1 of 31 patients (3.2%) with severe sepsis and in none of the patients in septic shock. Overall mortality was 37% (severe sepsis 29%, septic shock 46%).
Conclusion: In this urban ED, CVP monitoring was uncommonly used in patients presenting with severe sepsis or septic shock. Monitoring IVC respiratory variation by US is a useful alternative technique to guide fluid resuscitation in these patients, but was used even less (in only 1 of 57 patients). The under-utilization of these techniques was associated with inadequate fluid therapy and a high mortality rate. Implementation of IVC US training for resident physicians and formal integration within ED sepsis management protocols can improve outcomes for these critically ill patients.
10. Emergency Department Central Line Associated Blood Stream Infections (CLABSI) Incidence in the Era of High Prevention
Daniel L. Theodoro1, Margaret A. Olsen1, David K. Warren1, Kathleen M. McMullen2, Phillip Asaro1, Adam Henderson1, Michael Tozier1, Victoria Fraser1. 1Washington University School of Medicine in St. Louis, St. Louis, MO; 2Barnes Jewish Hospital, St. Louis, MO
Background: The incidence of central line associated blood stream infections (CLABSI) among central venous catheters (CVC) inserted in the Emergency Department (ED) is not well tracked or reported.
Objectives:Our goal was to determine the rate of ED CLABSI during an era of increased focus on CLABSI prevention practices.
Methods: This was a prospective observational study over a 28-month time period from March 2008 to June 2010 at a single academic tertiary care center. After month 13 a CVC insertion bundle was introduced hospital-wide by infection prevention to standardize insertion practices and prevent CLABSIs. Using the electronic ED health record, a standardized CVC procedure note was created to identify CVC insertions taking place in the ED. Trained abstractors reviewed ED records of patients with CVC to determine ED CVC catheter-days. Blood culture results up to 2 days after ED CVC removal were obtained from a hospital informatics database and an infection prevention specialist identified CLABSIs originating in the ED using National Hospital Safety Network definitions. ED CLABSI rates were compared to institutional CLABSI rates collected by infection prevention for routine surveillance. Administrative data, also obtained from the hospital informatics database were used to determine the sensitivity of billing data in identifying CVCs inserted in the ED. Results were analyzed using proportions and 95% confidence intervals.
Results: The ED CLABSI rate was 2.0/1,000 catheter days (95% CI, 1.0 to 3.8). The concurrent institutional composite intensive care unit (ICU) CLABSI rate was 2.3/1,000 catheter days (95% CI 1.9-2.7). Eight CLABSIs occurred before the introduction of a CVC prevention bundle and 1 occurred after. Clinical Procedural Terminology (CPT) codes detected 74% (95% CI 71-77%) of CVCs inserted in the ED and International Classification of Diseases, 9th edition (ICD-9) procedure codes detected 57% (95% CI, 53-59%); together CPT or ICD-9 codes detected 88% (95% CI, 86-90%) of ED CVC insertions.
Conclusion: Composite ED CLABSI rates were in the range of those reported by the ICUs. Combining hospital and physician billing information improves the sensitivity of administrative data. Further research dedicated to surveying ED CLABSI rates are necessary to determine the impact of CLABSI prevention practices in the ED.
11. Early Goal-Directed Therapy Compliance in Patients Transferred with Severe Sepsis or Septic Shock to a Large Academic Hospital
Joseph Noack, Nicholas Mohr, Brett Faine, Terrence Wong, Azeemuddin Ahmed. University of Iowa, Iowa City, IA
Background:Sepsis is a life-threatening condition that relies heavily on early recognition and treatment. Early goal-directed therapy (EGDT) has decreased the mortality rate of sepsis nearly 25% in the last two decades. Many patients in rural areas who present with sepsis are transferred to a larger hospital to receive specialized care. The question of whether inter-transfer interrupts the delivery of early goal-directed therapy has not yet been answered.
Objectives: The aim of the study was to identify if inter-hospital transfer from rural institutions to larger institutions results in delays in time sensitive care for patients with severe sepsis or septic shock.
Methods: A retrospective cohort analysis was conducted on patients who presented to the University of Iowa Hospitals and Clinics (UIHC) Emergency Department (ED) with severe sepsis or septic shock following transfer from a regional hospital from 2009-2014. Patients who presented directly to the UIHC ED served as controls. Comparisons of treatment times were analyzed with chi-square and two-tailed t-test calculations to identify differences in care between the two cohorts.
Results: Data was collected from 38 transfer patients and 135 control patients. Patients with an abdominal (p=0.010) or necrotizing fasciitis (p=0.003) source of sepsis were more likely to be transferred, while patients with pneumonia were less likely to be transferred (p=0.028). The transfer patients were more likely to get surgery while at UIHC (p<0.001), but only 55.3% of the transfer patients needed surgery. Transfer patients spent more time in the ED before being admitted to the inpatient unit (10.36±6.0 hours vs. 4.18±1.95 hours, p=0.001). While in the ED, transfer patients were more likely to receive adequate fluid resuscitation (p=0.031), receive vasopressors (p=0.03), and have placement of a central venous catheter (p=0.008). The time to first antibiotic in the study group was 3.23±3.28 hours compared to 2.05±1.42 hours in the control group (p=0.042).
Conclusion: Inter-hospital transfer leads to significant treatment delays in patients with severe sepsis and septic shock. Future studies should evaluate interventions to increase the early recognition and treatment of sepsis patients presenting to rural hospitals.
12. The Recognition of Hospice Eligible Patients In The Emergency Department: A Missed Opportunity
Melissa Bacci, Karisa Harland, Adam Schlichting, Andrew Nugent. The University of Iowa, Iowa City, IA
Background: Integrating palliative medicine and hospice services into emergency medicine is essential to providing optimal patient care, yet it remains unknown how well emergency department (ED) clinicians recognize hospice eligible patients. Early recognition of these patients in the ED could lead to more timely access to palliative care (PC) that could substantially improve their quality of life.
Objectives: To identify hospice eligible ED patients based on current guidelines and to determine whether they were identified and treated as such by the ED treating staff.
Methods: A retrospective chart review was completed for all ED visits of adults 65 years of age and older at a large academic medical center from September-November 2013. Physician and social work notes, including those from the ED visit, were evaluated for hospice eligibility using criteria from the National Hospice and Palliative Care Organization and Medicare guidelines. Hospice eligibility was evaluated, as no objective measure to assess PC eligibility exists. To examine recognition of hospice eligibility, the occurrence of PC discussions in the ED, PC consults initiated from the ED, and hospice referrals for eligible patients were recorded. Patients already enrolled in hospice were excluded.
Results: Out of 1884 ED visits reviewed, 237 visits (12.5%) were by patients that met hospice eligibility criteria. Almost half of these visits (n=114, 48%) were by patients who had been seen in the ED in the previous 12 months, and of those with prior visits, 50% (n=58) had multiple visits. PC discussions were documented in 7.6% (n=18) of visits. Among those with PC discussions, over half (10 of 18) did not receive a PC consult or hospice referral from the ED.
Conclusion:The majority of hospice eligible ED patients 65 years of age and older went unrecognized in the ED and had no documented PC discussion. Even among those with a discussion, many received no consult or referral. As a result, only a fraction of patients who may have benefitted from PC were offered the opportunity to utilize it. Our findings illustrate the importance of educating ED staff, as well as creating automated electronic tools that alert staff to potential hospice eligible patients. Improving the recognition of these patients may lead to more timely and appropriate use of PC services that in turn, provide the highest quality of care to these patients and their families.
13. MINI Kid Study: Emergency Department Screening for Psychiatric Illness in Pediatric Patients
Jacqueline L. Nguyen1, La Vonne A. Downey2, Trena M. Burke1, Leslie S. Zun1. 1Chicago Medical School, North Chicago, IL; 2Roosevelt University, Chicago, IL
Background:Pediatric mental health disorders currently afflict 21-23% of children and adolescents in the US. Adolescents frequently visit the Emergency Department (ED) because many do not have access to a primary care provider. However, up to 98% of mental health problems in pediatric patients go undetected by ED physicians.
Objectives: To identify unsuspected psychiatric illness in adolescent patients who present to the ED with non-psychiatric complaints using a validated survey tool: the MINI International Neuropsychiatric Interview for Children and Adolescents (M.I.N.I. KID) and to evaluate the effectiveness of referrals administered.
Methods: After patients assented and parents/guardians consented, all patients (ages 12-17) with non-psychiatric complaints were enrolled and interviewed using the MINI Kid. ED physicians were notified of patients who tested positive for mental illness and patients were referred to a mental health worker for evaluation. After discharge, patients were contacted to follow-up regarding their psychiatric treatment. Data was analyzed using SPSS version 21. This study was IRB approved.
Results: A total of 175 patients were enrolled, the majority consisted of 56.6% African American and 42.3% Hispanic. Using the MINI Kid, 44.6% (78) of patients tested positive for 1 or more modules. Of patients who tested positive for mental disorders, 35.9% (28) tested positive for 1 module, 16.7% (13) tested positive for 2 modules and 47.4% (37) tested positive for 3 or more modules.
The most common modules are: Major Depressive Episode Current - 6.3% (11), ADHD Combined - 5.7% (10), Agoraphobia without History of Panic Disorder - 4.6% (8), and Oppositional Defiant Disorder - 4.0% (7). Of those who tested positive, only 10.3% (6) of patients used any services; but the majority of patients who contacted resources, found the referrals helpful.
Conclusion: The MINI Kid Interview is a beneficial tool to screen ED pediatric patients for undiagnosed mental disorders. However, ED patients exhibit low compliance to utilize referrals to receive proper psychiatric aid. Further studies should be conducted to improve patient adherence to mental health referrals and follow-up. Early mental health screening for psychiatric illness is vital to identify mental disorders in patients and improve overall long-term health outcome.
14. Assessment and Referral for Treatment of Patients at Risk for Suicide in the Emergency Department
Paul Vithayathil1, Trena Burke2, LaVonne Downey3, Leslie Zun1. 1Chicago Medical School at Rosalind Franklin University, North Chicago, IL; 2Mt. Sinai Hospital Emergency Department, Chicago, IL; 3Roosevelt University, Chicago, IL
Background: ED visits for suicide attempts have increased by 47% in the last 10 years. 40% of completed suicides among individuals over 16 years were seen in the ED one year before. Screening in ED could potentially capture these patients.
Objectives:Identify patients with non-suicide related illness presenting to the ED who might be at risk for suicide and refer them to appropriate services.
Methods: We sought to enroll 300 patients by convenience sampling in the ED of a Midwest urban level 1 trauma center. Subjects were consented and administered the Columbia-Suicide Severity Rating Scale (C-SSRS) to determine if it identifies patients at risk for suicide. The C-SSRS has 6 questions, has been validated for use in the ED, and administration takes less than 5 minutes. Inclusion criteria were all consenting English speaking medically stable patients. Exclusion criteria were patients who are not medically stable, do not give consent, and are non-English speaking. Data was analyzed by SPSS (ver. 14, IBM).This was an IRB approved study.
Results: 300 patients were enrolled by convenience sampling. The sample demographics were as follows: 56.7% (170) female, 75.7% (227) African American, Average Age: 37.03 (std. dev. 15.820)
The C-SSRS was effective in identifying patients at risk for suicide. 19% (57) of patients screened positive. Of the positives, 70% (40) had past suicidal behavior, and 14% (8) had current thought, intent, plan, and method. Psychiatric complaints represented 100% (5) of cases with positive current suicidal intent and method in the 18-21 (2) and 45-54 (3) age range (F=1.952, p= 0.011). Current suicidal ideation was higher in females than males (3.6% (6) vs. 1.6% (2) of all cases).
Conclusion: Consistent with previous studies showing females and younger patients as higher risk. The C-SSRS identified patients with psychiatric disease with highest risk of current suicidal ideation. We recommend screening psychiatric patients for current suicidal ideation and intent. Musculoskeletal complaints were correlated with past suicidal behavior in young patients and respiratory complaints were associated with elderly patients. Because past suicidal behavior is a major risk factor for future attempts, we recommend screening younger patients with musculoskeletal complaints and elderly patients with chronic respiratory issues.
15. Reasons for Psychiatric Readmissions to the Emergency Department
Loryn Wilson1, Leslie Zun1, Trena Burke1, LaVonne Downey2. 1Mt. Sinai Hospital - Rosalind Franklin University, Chicago, IL; 2Roosevelt University, Chicago, IL
Background:Emergency Departments (EDs) have become increasingly overcrowded and this has the potential to impact quality and accessibility of care. Frequent users of the ED contribute to the problem of overcrowding and are more likely to have psychiatric problems. In addition, ED visits due to mental health problems have increased in recent years.
Objectives: To determine the reasons for return ED visits of psychiatric patients.
Methods: This is a retrospective chart review of a random sample of 350 psychiatric patients who presented to the ED and had a return visit within 90 days. This study was conducted at a 432 bed, urban, level I adult and pediatric trauma center with 50,000 ED visits per year. The inclusion criterion was all psychiatric patients who presented to the ED since January 2010 and had a least one return visit within 90 days. The exclusion criterion was patients who presented with non-psychiatric complaints. SPSS version 14 was used, and the study was IRB approved.
Results: The most common psychiatric diagnoses for each of three visits within 90 days were depression, schizophrenia, schizoaffective disorder, bipolar disorder, and psychosis. The most common reasons for the second visit were 1. Psychiatric (61.9%), 2.Musculoskeletal (9.2%), 3.Cardiovascular (5.7%), 4. Neurological (4.3%), and 5. Dermatological (3.2%) complaints while the most common reasons for the third visit were 1. Psychiatric (55.4%), 2.Musculoskeletal (7.0%), 3.Drug/alcohol abuse (7.0%), 4.Neurological (6.1%), and 5. Dermatological (4.6%) complaints. ANOVA analysis showed that there was a significant difference in the reasons for the second and third visit (p = 0.001). The admission rate for each visit was 51.4% for the first, 44.1% for the second, and 35.5% for the third.
Conclusion: Psychiatric patients are not returning to the ED repeatedly for the same complaints or for only psychiatric complaints. Musculoskeletal complaints were the most common reason for return (after psychiatric complaints), and depression was the most common psychiatric complaint observed.
16. Utilization of the ED for Violence Prevention Referrals
Nicholas Leader1, Leslie Zun1, LaVonne Downey2, Trena Burke3. 1Chicago Medical School, Rosalind Franklin University of Medicine and Science, North Chicago, IL; 2Roosevelt University, Chicago, IL; 3Department of Emergency Medicine, Mount Sinai Hospital, Chicago, IL
Background:The rate of violence in the inner city population is at epidemic proportions. Homicide is the second leading cause of death for youth in the US between the ages of 15-24, with over 82% of these cases being attributable to firearms. Many of these victims present to the Emergency Department for treatment, which previous studies have found to be an effective location for patient intervention.
Objectives: The purpose of this study is to determine the effectiveness of an ED-based violence prevention referral.
Methods: A convenience sample of medically stable patients aged 16-24 years old presenting to the emergency department as victims of interpersonal violence were eligible. The study was conducted at an urban, teaching level 1 trauma center. After patient consent was obtained, a violence prevention brochure containing available referral sources was provided. Participants were contacted after discharge by their preferred method: phone call, text message, or email. Data was analyzed using SPSS version 14. This study was approved by the IRB.
Results: Two hundred thirty-six victims of interpersonal violence that met the criteria were enrolled in the study. The average age was 20.5 and 81.8% were male. Of those enrolled, 71.6% were African American and 25.8% were Hispanic. Gunshot wounds accounted for 59% (n=141) of the diagnoses.
Phone call was the preferred method of contact for 86.4% of the patients, followed by text message (7.2%) and email (6.4%). Nearly half (49.2%, n=116) of the first follow up attempts were successful, while 14% (n=33) of the second attempts were achieved. Overall, only 10.6% (n=25) of the patients enrolled in the study utilized the referral brochure. The top three resources that were contacted include: anti-violence victim hotline, job training, and financial service.
Conclusion: Providing a brochure with referrals to victims of violence is not a very effective ED intervention strategy, although majority (76%, n=19) that did contact the resources found them to be helpful. Alternative forms of intervention should be tested, considering that victims of violence have an alarming rate of recidivism in conjunction with more aggressive retaliatory attitudes.
17. Changes in Emergency Department Volumes in Winter 2014
Hans House, Ben Oglivie. University of Iowa - Carver College of Medicine, Iowa City, IA
Background:Emergency department (ED) visits can be affected by weather and changes in access. In 2014, the Affordable Care Act was fully implemented. The American College of Emergency Physicians (ACEP) conducted a poll in April 2014 asking members about changes in ED patient volume, number of Medicaid patients, and acuity of visits seen in the first three months of 2014.
Objectives: The aim of this study is to examine for regional differences in emergency department visits and payer mix for the first quarter of 2014 (January - April).
Methods: We obtained the raw data of the ACEP poll. We analyzed the data collected from all 50 states focusing on emergency department visits and payer mix. We then categorized the 48 contiguous United States regionally by using the National Climatic Data Center (NCDC) nine climatically consistent regions, which was assembled to put climate anomalies into a historical perspective.
Results: The poll was conducted from April 4 - 14, 2014, with 1845 physicians polled and a 8% response rate. Collectively, 46% of respondents report an increase in ED volume, 27% report no change, and 23% report a decrease in volume. A plurality report an increase in volume in every region except the Upper Midwest (IA, MI, MN, WI). There, 22% report an increase, 30% report no change, and 42% report a drop in ED census. The largest increases in patient volume were seen in the West region (66%). Collectively, most ED’s report more Medicaid patients and fewer privately insured patients. There was no difference in changes to payer mix by climate region, but ACEP’s own analysis found that states that expanded Medicaid saw an increase in Medicaid patients.
Conclusion: There were significant differences in reported volume changes regionally. Since the implementation of the Affordable Care Act (ACA), most ED’s have seen an increase in the number of patients, especially in states that expanded Medicaid coverage. But the Upper Midwest, on the average, saw a drop in the total number of patients. This may be due to the abnormally cold winter experienced this year. However, the Northeast experienced a very cold winter as well and 41% experienced an increase in census.
18. Comparison of Interpreters in the Emergency Department
Jason E. Smith1, Trena M. Burke1, LaVonne Downey2, Leslie S. Zun1. 1Chicago Medical School, North Chicago, IL; 2Roosevelt University, Chicago, IL
Background:Communication barriers between emergency department (ED) staff and limited English proficiency (LEP) patients have fundamental impacts on patient care and satisfaction. As LEP patients are a significant and growing minority of those seen in the ED, continual evaluation of different interpretation methods is needed.
Objectives: To determine the effects of three different interpretation modalities with regards to patient satisfaction and understanding, health care provider satisfaction, length of stay and cost of care in the ED.
Methods: This study occurred at an inner city level one trauma center with 60,000 ED visits per year. Medically stable Spanish speaking patients, 18 years and older, presenting to the ED were enrolled. After consent, patients received one of three different interpreter services: a hospital provided interpreter (LIVE), physicians/nurses that spoke Spanish, or a videoconferencing technology (IVIN).
Patient satisfaction and understanding, and health care provider satisfaction were assessed with a brief survey. Statistical analysis was performed with SPSS (ver. 14, IBM). ANOVA tests were used to determine statistical significance. A p value < 0.05 was considered statistically significant.
This study was IRB approved.
Results: A total of 82 patients were enrolled. Of those, 99% were Hispanic and 52% were female. Average age was 49 (SD 17.4). 43 patients used hospital provided interpreters, 20 patients had a Spanish speaking physician or nurse and 19 used the videoconferencing technology, IVIN.
There were no significant differences between reported patient satisfaction, patient ease of understanding, or health care provider satisfaction between groups.
Additionally, there were no significant differences in length of stay or total charges between groups. Finally, there was no association between type of interpreter service used and assessed patient acuity.
Conclusion: Providing interpreter services to Spanish speaking LEP patients resulted in high degrees of patient satisfaction and understanding, regardless of modality.
Additionally, this study demonstrated that an on-demand videoconferencing interpreter system could be part of the solution to providing sufficient interpreter services to LEP patients.
19. A Collaborative Approach to Reducing Emergency Department Overcrowding
Erin Willard, Seamus Murphy, Elizabeth Carlton, Bradley E. Barth. University of Kansas, Kansas City, KS
Background: Emergency department (ED) overcrowding is a national issue.
Objectives:After previously reporting on the effectiveness of using an ED Flow Coordinator to improve patient throughput, we developed a plan known as the Full Capacity Protocol (FCP). The FCP is a pre-determined response that calls for leaders from various departments to descend on the ED and collaborate to identify and remove barriers to patient flow. The goal is to create a system in which patient admission is a safe, fluid process that involves equal ED pushing and hospital pulling to achieve optimal outcomes. This study examined the effectiveness of the FCP in achieving that goal.
Methods: This retrospective observational study examined various hospital and ED metrics before and after implementation of the FCP. We compared the first six months the protocol was in use to the corresponding six months from the year prior to implementation. Two analyses were performed: one that examined cumulative data during these time periods and one that compared days on FCP in 2014 to similar days in 2013 (Prior to FCP). Statistical significance was measured using two-sided t-tests. Binomial proportion confidence intervals were calculated using the Wilson score interval method.
Results: The cumulative analysis showed a 7.4% increase in ED encounters (p<0.001) and an 11.9% increase in ED admissions (p<0.001) compared to the corresponding time period in 2013. The ED also saw a 10.2% decrease in total LWBS that was not statistically significant (p=0.29), an increase in LOS of 34 minutes (p<0.001), and a 92% decrease in ambulance diversion (111 fewer hours). In the second analysis, the 27 days on FCP were compared to similar days (matched by volume and acuity) from the previous year. Similar the LOS was higher for FCP days (p<0.001). The LWBS rate subsequent to FCP activation was less (p<0.05) than that of similar days from the previous year. On days the FCP was activated, the rate of hospital admissions was increased (p<0.05).
Conclusion: A FCP is effective in reducing LWBS, ambulance diversion, and accommodating increased hospital admission rates while also allowing for a significant increase in ED volume. This indicates that a multidisciplinary approach can generate substantial improvements in a hospital’s ability to address ED overcrowding and patient throughput.
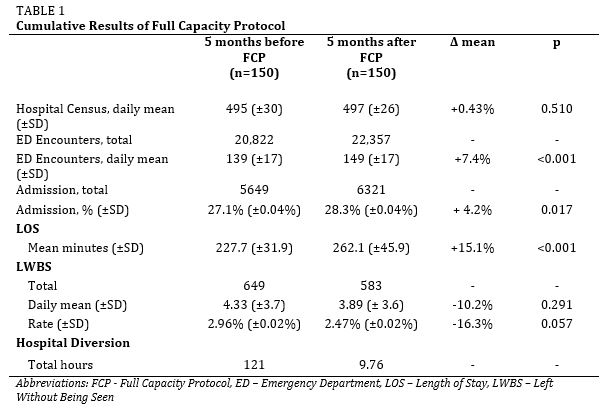
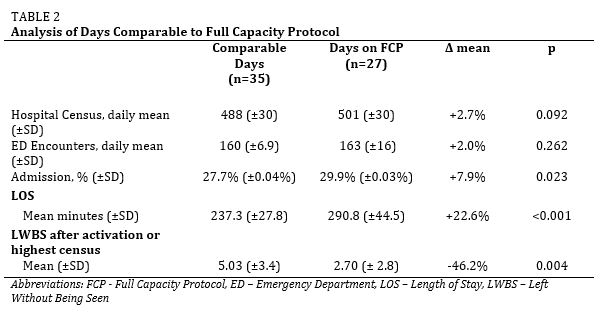
20. The Impact of an Emergency Department Observation Unit on Patient Throughput: A Before and After Analysis
Parker D. Rayl, Seamus O. Murphy, Bradley E. Barth. University of Kansas, Kansas City, KS
Background:In 2011, the total number of emergency department (ED) visits in the U.S. was over 131 million; nearly 9% higher than in 2006. Observation units (OU) address this overcrowding issue and serve as an alternative option for various patient populations who would otherwise be admitted, providing financial savings and increased ED throughput.
Objectives: A Clinical Throughput Unit (CTU) was implemented at our institution in September 2013 to serve patients meeting standard OU criteria, but also to relieve the ED in times of overcrowding. The CTU was open M-F, giving us an opportunity to use Sat-Sun as a pre/post control.
Methods: Data were analyzed by day of week and corresponding months were chosen to account for routine variations in volume. Throughput metrics before and after the introduction of the CTU provided for an analysis of any change exclusively during operational hours. Statistical significance was measured for each variable using two-sided t-tests and Wilcoxon Rank-Sum tests, and confidence intervals were calculated using the Wilson method.
Results: Comparing Monday-Friday (M-F) before and after CTU implementation, LWBS was reduced by 118 (p=0.01, CI± 2.8) or 0.86% (p=0.004, CI±0.2%), diversion was reduced by 8.4 minutes (p=0.49, CI±0.08), and total ED volume increased by 701 (p=0.06, CI±36.4). In our control group, comparing Saturday-Sunday (S-S) before and after, there were no significant changes in LWBS totals (increased by 2, p=0.45, CI±0.65), LWBS percentage (dropped by 0.13%, p=0.29, CI±0.3%), or diversion (increased by 3.49 hours, p=0.17, CI±0.21). Total ED volume increased by 448 (p=0.02, CI±12.4).
Conclusion: A CTU, staffed by ED physicians, is effective in achieving reductions in LWBS rates and diversion hours despite increases in ED volume, in addition to providing all the fiscal benefits of an OU.
21. Potential Return on Investment for an Academic Emergency Department Ultrasound Program
Ernest S. Mavunga, Janet S. Young, Kim E. Roe. Virigina Tech Carilion Clinic, Roanoke, VA
Background:Maintaining an emergency medicine ultrasound training program hashistorically been expensive due to costs associated with faculty salaries, infrastructure and ongoing equipment replacement. The use of ultrasound in the emergency medicine has increased dramatically over the past 3 decades as point-of care ultrasound has improved the care of emergency patients, and subsequently, was declared a necessary skill for emergency physicians by the emergency medicine governing boards. Applications of point-of-care ultrasound that have been highlighted by the governing and educational boards include: thoracic-abdominal trauma, ectopic pregnancy, abdominal aortic aneurysm, pericardial effusion, cardiac arrest, biliary disease, renal tract disease, and procedural guidance.
Objectives: This project set out to investigate the return on investment for ultrasound procedures in the emergency department based on current Medicare reimbursement guidelines.
Methods: Ultrasound exams performed in our emergency department that were logged in an electronic archival system over a 2 month period were analyzed and results extrapolated to estimate the potential reimbursement from point of care ultrasound in 5 years, the expected duty life of an ultrasound machine.
Results:
With an expected 4000 ED studies for an 80,000 visits/year billing profile, our academic emergency department ultrasound program could provide revenue in excess of costs within the first year of program inception.
Conclusion:
The use of ultrasound in the ED is a viable and sustainable financially based on current medicare reimbursement guidelines, if using an an expected 4000 ED studies for an 80,000 visits/year billing profile.
22. Patient Care Intervals Associated With Increased Productivity
Brian Roach1, Logan H. Stuck2, Michael Zwank1. 1Regions Hospital, Saint Paul, MN; 2Healthpartners Institute for Education and Research, Bloomington, MN
Background:Emergency department crowding is a recognized barrier to delivering timely care in the US. A review of the literature identifies 71 separate measures of crowding. This review suggests that the time interval of ED length of stay (LOS) is an important crowding variable. Dividing ED LOS into more discrete time intervals may allow for a better analysis of this variable.
Objectives: This study analyzed the relationship between emergency department provider productivity and its relationship to specific time intervals during a patient’s LOS. We aimed to determine which time intervals have the greatest variability between providers, perhaps indicating a target for intervention to decrease LOS.
Methods: This retrospective chart review was approved by the IRB. We collected data from the EMR during 6 months from an area of the ED where attendings see patients without residents or PA. Data collected included provider productivity variables of RVU/hour and patients/hour. Patient data included age, means of arrival, labs ordered, imaging ordered, consultations ordered, procedures and treatments. LOS was divided into intervals based on time stamps of triage, placement in room, initiation of treatment (provider signs up for the patient), placement of first order, placement of disposition order and departure.
Results: There were 421 patients seen by 28 providers. Mean age of patients was 35. 56% of patients had labs, 40% had imaging, 89% had an EKG, 4% had consultations and 6% had procedures performed. After regression analysis, each unit of RVU/hr increase was associated with a 6% decreased in the patient LOS (95% CI 2% to 9%, p=0.001). Procedures, EKG, day of week, arrival means, age and sex did not alter this. The two intervals that showed significant correlation with productivity were time of patient rooming to begin of treatment phase when the provider signed up for the patient and first order placed to disposition order. There was no difference in presentation at triage to rooming, treatment phase to first order and disposition to departure.
Conclusion: As one would predict, provider productivity/efficiency impacts length of stay. The intervals that showed significant difference were rooming provider signing up for the patient and first order until disposition order. This suggests the importance of initiating care.
23. Does an Electronic Medical Record Alert Affect Door to Antibiotics Time in Four Community Hospitals?
Michael D. Zwank. Regions Hospital, Saint Paul, MN
Background:Sepsis is a leading cause of mortality in the United States. Early initiation of appropriate antibiotics has been shown to improve outcomes and decrease mortality. Systems based interventions to quicken the administration of antibiotics are an attractive goal to improve quality of care.
Objectives: As part of a quality improvement project, we sought to determine if an automatic prompt in the electronic medical record (EMR) or use of a sepsis order set was associated with a decreased interval between patient arrival and administration of antibiotics (Door to Antibiotics).
Methods: A single group staffs the emergency departments at four community hospitals of various sizes in the region surrounding St. Paul, Minnesota. All of these hospitals share the same EMR. Two years ago, we instituted an automatic prompt to alert providers when a patient arrived with or developed vital signs consistent with systemic inflammatory response syndrome (SIRS) as well as an order set prompting providers to order accepted care items such as labs, fluids and antibiotics. Allowing a period of accustomization, we collected data over one year to determine if there was a difference in time to antibiotic administration when the prompt was given or when providers used the order set.
Results: There were 147 patients (average age 70, 50% male) seen by 35 providers. Mean door to antibiotics was 125 minutes (range 9-370). 26% of patients received antibiotics within 60 minutes, 55% within 120 minutes and 82% within 180 minutes. 96 patients had the SIRS prompt given by the EMR because they met criteria. 56 patients had the sepsis order set used. The SIRS alert did not affect the percent of patients receiving antibiotics at any time interval. Patients who had the order set used had a non-statistical trend towards receiving antibiotics within 60 minutes (32% versus 23%; p=.252) but not within 180 minutes.
Conclusion: At these community hospitals, there is no association between prompting physicians that a patient meets SIRS criteria and time to antibiotics. There is a trend towards improvement in patients receiving antibiotics within 60 minutes when a sepsis order set is used. Future efforts could examine similar data pre- and post-intervention. It is possible that the prompts and order set have improved sepsis awareness and timeliness of care.
24. Faculty Prediction Of In-training Examination Scores Of Emergency Medicine Residents: A Multi-center Study
Erin N. Quattromani1, Amer Z. Aldeen2, Kelly Williamson3, Nicholas D. Hartman4, Natasha B. Wheaton5, Jeremy B. Branzetti6. 1St. Louis University School of Medicine, St. Louis, MO; 2Presence St. Joseph Medical Center, Chicago, IL; 3Advocate Christ Medical Center, Chicago, IL; 4Wake Forest School of Medicine, Winston-Salem, NC; 5University of Iowa Carver College of Medicine, Iowa City, IA; 6University of Washington School of Medicine, Seattle, WA
Background:The Emergency Medicine In-Training Examination (EMITE) is one of the only valid tools for medical knowledge assessment in current use by emergency medicine (EM) residencies. However, the EMITE results return late in the academic year, providing little time to institute potential remediation. A single site study found moderate accuracy of faculty to predict resident EMITE scores.
Objectives: To measure the ability of EM faculty to accurately predict resident EMITE scores prior to the return of results at multiple institutions.
Methods: Five different institutions received IRB approval or exempt status. We asked EM faculty at these five different residency programs to predict 2014 EMITE scores of their residents prior to the actual exam. The primary outcome was prediction accuracy, defined as the proportion of predictions within 6% of actual score. The secondary outcome was prediction precision, defined as mean deviation of predictions from actual scores. We assessed several faculty background variables, including years of experience, educational leadership status, and clinical hours worked, for correlation with the two outcomes.
Results: At five different programs, 111 total faculty physicians participated in the study rendering 3,219 predictions for 147 residents (response rate 68.9%). Mean resident EMITE score was 78% (95% CI 71-82%). Mean prediction accuracy for all faculty participants was 60% (95% CI 57.5-62.6%). Mean prediction precision was 6.3% (95% CI 6.0-6.6%). Prediction accuracy was not significantly different between educational leaders (63.9% 95% CI 60.4-67.4) and non-educational leaders (58.4%, 95% CI 44.2-61.6) or correlated with any other faculty background variables. Eight participants predicted scores with high accuracy (>80%). Individual site data for residency size, faculty size, and ITE scores were not reported in order to maintain optimal confidentiality for the residency programs.
Conclusion: In this multicenter study, EM faculty possess only moderate accuracy at predicting resident EMITE scores. This calls into question the ability of faculty (including educational leadership) to accurately assess a standardized marker of medical knowledge.
25. Inaugural UMKC All Health Profession Schools Interprofessional Education Class: It is Everyone's Role and Responsibility to Provide Safe Patient Care
Stefanie Ellison, Megan Litzau, Linda Garavalia, Jennifer Quaintance. University of Missouri-Kansas City, Kansas City, MO
Background:Interprofessional education (IPE) is defined as opportunities where students from two or more different professions learn with, about, and from one another to practice as a team to provide safe, patient-centered care. The IPE collaborative was founded in 2009 and defined 4 competency domains: Roles and Responsibilities, Ethics and Values, Communication Skills and Teams and Teamwork to provide a framework to professional schools to increase curricular activities in IPE.
Objectives: The objectives of this activity were to develop student understanding of other professionals’ roles and responsibilities and to begin to practice providing safe patient care on teams.
Methods: In the inaugural IPE instructional activity at UMKC over 620 students convened for learning on the domain of Roles and Responsibilities with a focus on patient safety. Students met in Interprofessional Medical Patient Advocacy and Collaborative Teams (IMPACT) of 10 learners from 6-8 different health professional programs from the UMKC and UM -Columbia campuses. In Kansas City, 570 students from SOD, SOM, SONHS, and SOP convened in IMPACTs while the Columbia campus IMPACTs were from their SOP, SON, and PT. The class activities included an IPE and patient safety lecture; individual writing on Roles and Responsibilities; facilitated small group case-based learning; and an achievement test. Students also completed a survey on the instructional activities and pre- and post- IPE attitudes.
Results: 69% of students agreed or strongly agreed that the IPE class was a good experience and a similar 68.2% agreed or strongly agreed that the small group experience was beneficial. Of the 261 survey participants, 106 students provided written comments. Students commented on their enjoyment of working with other health care fields (24) and specifically on the impact IPE can have on patient safety (4). Plans for future IPE exercises: 1) increased time to work within small groups and 2) redesign the case for SOD students.
Conclusion: IP teams are now necessary to provide safe, high quality care in the practice setting. Every member of the healthcare team is responsible for patient safety and experiences in IPE are required to develop graduates who are practice ready. The inaugural UMKC IPE class and the development of IMPACTs was an important first step in meeting this call.
26. Emergency Medicine Interest Group Procedural Simulation Conference: A High Quality Experience for the Novice to Expert Learner
Stefanie Ellison, Megan Litzau, Emily Hillman. University of Missouri-Kansas City, Kansas City, MO
Background:The use of simulation in the training of medical students, EM residents and EM faculty has shown to be a useful aid. Medical students identified a knowledge gap between being able to verbalize steps in procedures and actual performance in simulation. Interactive simulation workshops alone or with other interventions are likely to improve performance compared with didactic lectures alone.
Objectives: The objectives for this conference are to introduce students to the procedure-based nature of EM, the interprofessional approach to EM care and to provide a model on which to build real-life skills before entering residency training.
Methods: This procedural simulation conference is designed to provide instruction with deliberate practice and structured feedback for skills development in learners of all levels. Each procedure station (Airway Management, Lumbar Puncture, Ultrasound, EMS, Suturing, and Trauma) has specific learning objectives for the skills as well as for the level of the learner to allow instructors to tailor the learning and practice to the level of student participating. Students have the opportunity for repetitive practice and feedback with procedurally competent residents, faculty and paramedics. The students are divided into groups of 10 or fewer medical students which will provide a student to instructor ratio of less than 5:1. The instructors will be a combination of EM faculty, residents and senior medical students entering the specialty of EM. Students will also experience interprofessionaleducation as paramedic and EMS instructors and paramedic students will be participating in instruction for an EMS station.
Results: Student performance will be assessed using skills checklists with feedback at each station. We will also survey student participants and faculty following the experience.
Conclusion: Due to the demands of performing high risk procedures under challenging conditions and the need for accountable and safe patient care, this procedural conference is a first step to develop procedural competence for student learners. It is also important that students are provided regular opportunities to develop and practice skills to become entrusted learners in preparation for residency and beyond. This conference is supported by a Society of Academic Emergency Medicine Foundation grant.
27. Bridging the Gap - Collaborative and Simulated M&M Conferences
Jason A. Kegg, Jonathan dela Cruz, James Waymack. Southern Illinois University School of Medicine, Springfield, IL
Background: Mortality and morbidity (M&M) conferences remain vital opportunities for learning and the avoidance of medical errors. We propose a novel and educationally innovative approach to the M&M conference by restructuring the format to a collaborative simulated patient encounter.
Objectives: We propose a framework to combine an M&M conference and a simulated patient encounter to evaluate not only the ACGME Competencies but also the American Board of Emergency Medicine (ABEM) Milestones. Such exercises could allow for further involved evaluation of resident competency in situational conditions and allow for the testing of teamwork skills and behavioral targets for assessment and feedback.
Methods: An adverse patient encounter in which an aortic dissection was treated as a myocardial infarction and anticoagulants were given, was kept confidential by the presenting resident and the case was written and structured as a simulated patient case. The overall goal of the simulation case was to assess, based on the patient’s presentation and limited historical and diagnostic information, whether 11 other residents would duplicate the error and pursue a diagnosis of acute myocardial infarction.
Results: This trial of collaborative simulation and M&M was performed with 11 residents. In this cohort, 7 diagnosed an AMI and 5 of those gave anticoagulants before the true diagnosis of aortic dissection was known. In the 4 situations where an AMI was not declared, the resident evaluated the patient for aortic dissection and obtained appropriate studies. In 3 cases, a chest x-ray was not obtained and in 1 case the study was ordered but not reviewed. Milestone assessment for PC1 and PC3 were generally consistent with the resident’s level of training. Feedback from the residents suggested this was a worthwhile educational activity and a collaborative activity was a valuable alternative to the traditional M&M presentation.
Conclusion: The integration of simulation with the M&M conference proved to be an enjoyable and useful educational experience allowing a novel opportunity to evaluate and debrief a clinical scenario outside of the confines of the traditional M&M conference. This provided additional insight into the resident’s thought process. The exercise also provided the faculty ways to assess the milestones in a direct observation manner.
28. An Innovative Approach to Junior Resident Introductory E-fast Education And Outcome Assessment
Michelle Clinton, Janet Young. Carilion Clinic, Roanoke, VA
Background:In many academic institutions junior residents perform the extended focused assessment with sonography in trauma (EFAST) exam during the trauma resuscitation. The inexperience of these residents and the urgency surrounding the care of trauma patients creates a high probability of error in the performance and interpretation of this crucial aspect of the trauma evaluation.
Objectives: This innovative approach to teaching the EFAST exam to novice sonographers aims to improve the accuracy and quality of EFAST exams performed by junior residents.
Methods: 18 junior residents were enrolled in 2 hours of intensive EFAST training. Residents completed a pretest assessing baseline understanding of the EFAST exam and indicated confidence level in their ability to accurately perform and interpret the EFAST exam on a visual analogue scale (VAS). Throughout a 45-minute lecture, twelve anatomic sites of ultrasound visualization crucial to a quality EFAST exam were repeatedly emphasized. Over 60 images or video clips of EFAST exams were displayed to reinforce this information. A one-hour scan lab followed, during which residents performed 2 supervised EFAST exams and were assessed on recognition of the twelve anatomic structures emphasized in the lecture. Residents completed a post-test and post-course VAS ranking confidence level in their ability to accurately perform and interpret an EFAST exam.
Results: Upon course completion, all residents performed EFAST scans better than expected for their level of training when assessed by 2 expert sonographers on a Likert scale. Participant exam score improved from a pretest mean of 58 percent to 80 percent on a post-test; demonstrating significant improvement in EFAST understanding. Learner confidence in EFAST scanning and interpretation ability increased 90% when pretest VAS rankings were compared to post course values.
Conclusion: A focused educational intervention emphasizing anatomic sites of importance in the EFAST exam, repeated EFAST image exposure, and supervised scanning improves the scanning ability, knowledge base, and confidence of junior residents. The effectiveness of this teaching protocol will be further assessed through evaluation of long-term knowledge retention and quality assurance review of junior resident EFAST exams prior and subsequent to the course.
29. A SMART Curriculum - Simulated Milestone Assessment for Residency Training - Standardizing The Assessment And Not The Patient
Jonathan dela Cruz, Jason A. Kegg. Southern Illinois University School of Medicine, Springfield, IL
Background:While the ACGME Milestones provide more explicit and transparent expectations of performance using competency-based outcomes, some Milestones are difficult to evaluate and require direct observation of resident performance. Such efforts performed in the ED are time intensive and somewhat informal. Simulation provides a platform where direct observation can occur in a more formal and educational setting but developing unique standardized cases that cover a variety of chief complaints is labor intensive and resource heavy.
Objectives: We propose an innovative simulation curriculum framework centered on a single standardized assessment form whereby chief complaint-based simulated scenarios can be implemented with minimal case development.
Methods: A standardized assessment form was developed evaluating 9 patient care, communication, and management milestones for PGY1 residents. Three different cases were written with the complaints of chest pain, abdominal pain, and weakness. A simulated construct was created where residents were observed in history taking, documentation, and planned orders for a case. The case and plan were then presented to an evaluating faculty. Residents then received word of a change in patient condition and were observed in their re-evaluation and disposition plan. Faculty built their cases in real time to comply with the assessment form. Feedback on the experience was then collected from both faculty and residents.
Results: Six residents and 4 academic EM faculty were involved in the experience. Overall, faculty found building the cases around the assessment form in real time helpful and easy. Faculty found they had a more active role in resident assessment by not having the constraints of a standardized simulation script, and could better assess resident performance with this added freedom. Residents found the experience enlightening and, in fact, gave feedback to have more assessments like this in the future.
Conclusion: Developing a simulation curriculum based upon a single standardized assessment tool rather than multiple unique standardized encounters allows for a novel method to obtain evaluation of resident Milestone performance. These patient care scenarios can be built with minimal developmental costs compared to building multiple standardized simulation scripts.
30. Preparing for Rare Events: Simulation of a Massive Variceal Bleed
Joseph W. Watkins, IV, Jason C. Wagner. Washington University in St. Louis, St. Louis, MO
Background:Variceal bleeding in a patient with liver cirrhosis is not uncommon. Rarely, however, when the bleeding is perfuse, we must undertake a rare but potentially life-saving procedure: the insertion of a Sengstaken-Blakemore tube. While the concept is simple, the insertion of the tube has many steps that must be performed both in series and in concert. This occurs in the setting of massive hemorrhage; not an ideal time to read instructions. The purpose of this study was to simulate the scenario of a massive variceal bleed requiring insertion of a Sengstaken-Blakemore tube, and to evaluate the resident’s knowledge of and comfort level with the procedure both before and after the simulation.
Objectives: To determine the effectiveness of Sengstaken-Blakemore insertion simulation among Emergency Medicine Residents in increasing knowledge and comfort level.
Methods: EM residents at an academic urban Level 1 trauma center were presented with a manikin posed as a patient with liver cirrhosis who presented with massive hematemesis. After voicing the need for Blakemore placement, the residents then attempted to insert the tube in a head-only model. 3 weeks after the simulation, an anonymous questionnaire was circulated with respondents answering questions on a 5 point scale regarding their level of training, how many Blakemore tubes had they placed, their familiarity with indications and the steps required for placement both before and after the simulation and their comfort level placing the tube before and after simulation. The change in values for pre and post simulation were evaluated for significance using the type 3 T test tool in Microsoft Excel. This study was approved by our IRB.
Results: 20 respondents completed the survey. One Blakemore tube had been placed in a patient prior to the study. Awareness of indications for insertion increased from 2.7 to 4.1 (p<0.001), awareness of steps required increased from 1.7 to 3.8 (p<0.001), and comfort level inserting a Blakemore tube increased from 1.5 to 3.4 (p<0.001).
Conclusion: Significance was achieved in improvement of knowledge and comfort for all of our measures. While these data need to be further tested, with serial simulations and evaluation with objective data, it appears that simulation of this life-saving and time-sensitive procedure improves knowledge and understanding among residents and should be implemented into curriculums.
31. Injury and Illness at Resident Summer Camps: An Evaluation For Improvement And Preparedness
Ross T. Miller, Bradley E. Barth. University of Kansas Medical Center, Kansas City, KS
Background: The purpose of this study was to examine the common illnesses and injuries that were sustained at a local resident camp.
Objectives:To identify areas of potential improvement and to make recommendations to increase the quality and preparedness of health services at resident camps.
Methods: We employed an observational study design to retrospectively analyze health center logbooks of a local resident camp. The logbooks included every visit to the health center and details about each visit such as the reason for visit, exam findings, treatment, and disposition. If a patient’s injury or illness involved multiple visits/rechecks, the subsequent visits were marked as “recheck”, but were given a new study ID. The study population was from H. Roe Bartle Boy Scout Camp in Osceola, MO from the summers of 2012 and 2013. Camp staff, youth and adult campers, visitors, and employees were included in the study population if they were seen in the Health Center. The logbook data was extracted into a digital database and placed into categories based upon the reason for the visit, treatments, and dispositions.
Results: 1,586 patients were seen at the health center during the 2-year study period. 67.0% were seen for an illness and 18.2% were seen for an injury. 91.1% of patients were considered safe to return to camp while 7.3% needed transfer to another facility and 0.9% were sent home. The most common reason for transfer was for radiologic imaging (35.7% of the total population that was transferred). The most common treatments were oral rehydration, oral medications, and topical creams. It was also found that EMS and hospital relationships had room for improvement of the provision of health services.
Conclusion: The data supported recommendations to increase efficiency and health outcomes by improving the available supplies and developing relationships with local EMS and hospitals was found in this study. Limitations to this study include the fact that this data only came from 1 camp from a period of 2 years. The logbook data was handwritten and limited secondary to the legibility of the writing and the level of detail based on the person logging the information. Also, this study did not account for injuries/illnesses that were self treated and thus not reported to the health center.
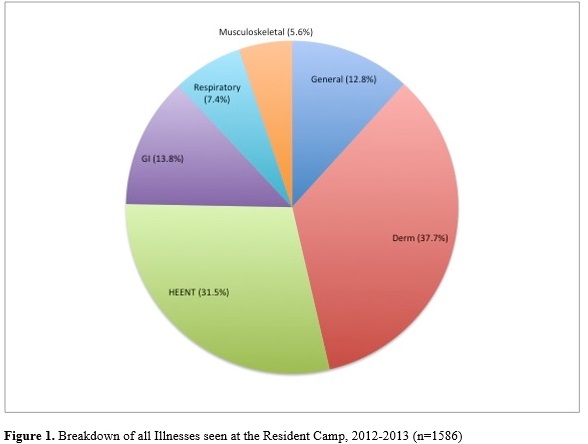
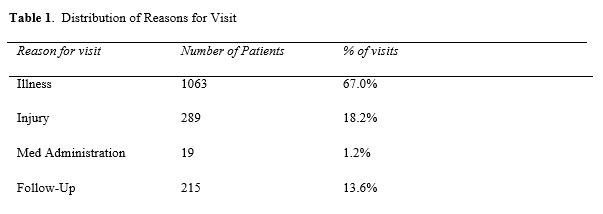
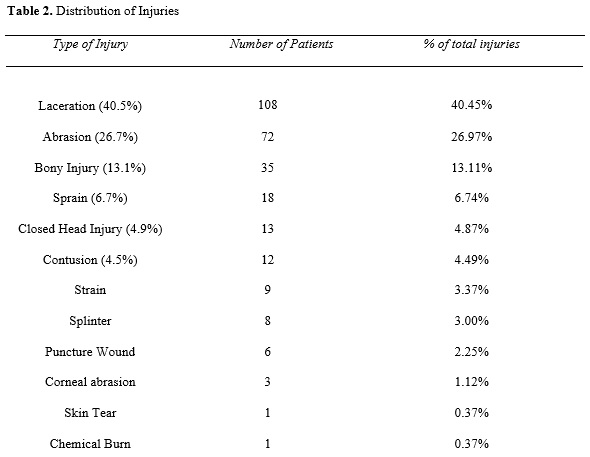
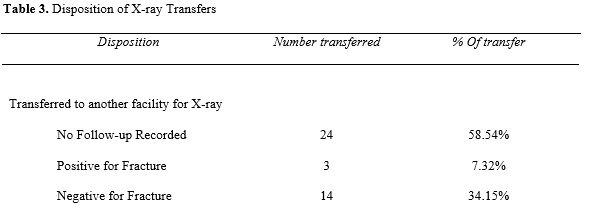
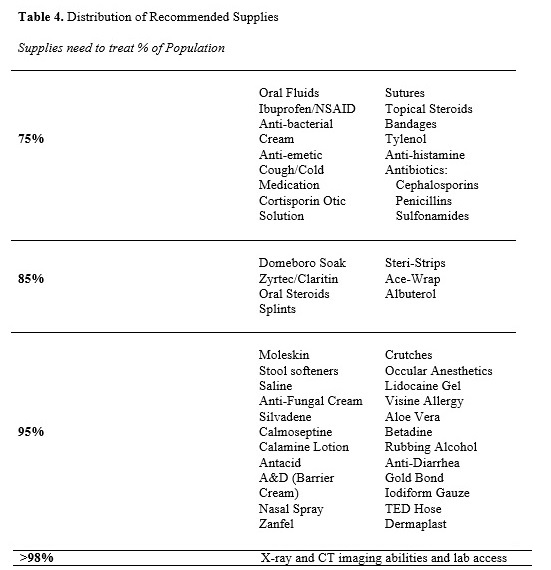
32. The Effect of Passengers on All-Terrain Vehicle Crash Mechanisms and Injuries
Charles A. Jennissen1, Joshua Godding2, Karisa Harland1, Gerene Denning1. 1University of Iowa Department of Emergency Medicine, Iowa City, IA; 2University of Iowa Carver College of Medicine, Iowa City, IA
Background: Traditional all-terrain vehicles (ATVs) are designed for one rider only. ATVs require “active riding,” meaning that the operator needs to assess changes in stability and rapidly adjust body position to compensate. Passengers likely alter the ability for drivers to actively ride and increase the center of gravity. Although passengers on ATVs are a known risk factor, how they contribute to crash likelihood and injury severity has not been well described.
Objectives: To better understand the effect passengers have on the mechanisms and injuries seen in ATV crashes.
Methods: A retrospective chart review and analysis was performed of ATV-related injuries from 2002-2013 at University of Iowa Hospitals.
Results: 538 cases were identified of which 20% were passengers or drivers with passengers. Both children and females were more likely to be passengers (p<0.0001). Although helmet use was low (~20%), drivers were more likely to wear helmets than passengers (p<0.01). Rollovers (49%) were the most common mechanism of injury. The victim was struck by their ATV in 19% and pinned in 10%. There was a trend seen that rollovers were more likely on sloped terrains with passengers. Backward rollovers were almost twice as likely to have passengers as all other rollovers and were also more likely to have passengers than non-rollovers. Victims who fell or were ejected to the rear were over seven times more likely to have been on an ATV with passengers than victims of other types of ejection (p<0.01) or those not ejected (p<0.01), and also had worse head injuries. Self-ejections and forward ejections appeared less likely if passengers were present. Patients who self-ejected had the highest extremity injury scores but less severe head injuries than other falls and ejections.
Conclusion: Passengers on ATVs may be at greater risk for fall/ejection to the rear which appears to increase the risk of head injury. ATV operators who self-eject receive extremity injuries but may be more able to protect their heads; passengers limit the ability of a driver to self-eject when losing vehicle control. A strict no rider rule could reduce risk of some ATV crashes.
33. All-Terrain Vehicle-Related Fatalities: All Roads Lead to Tragedy
Gerene Denning, Karisa Harland, Charles A. Jennissen. University of Iowa Department of Emergency Medicine, Iowa City, IA
Background: All-terrain vehicles (ATVs) are for off-highway use only, and many of their features create increased risk with roadway travel. They have deep-treaded tires designed to grab, rather than grip-and-release the road. Most have a locked rear differential or fixed rear axle, which means the back wheels do not turn at a different rate when going around a curve. Thus, ATVs require a relatively wider turning radius. ATVs also have lower pressure tires, a high center of gravity and a narrow track, all of which increase the risk of loss of control on roadways. Although the vast majority of ATV use is off-road, over 60% of ATV-related fatalities occur on roadways. Despite this, the epidemiology of ATV-related deaths on different road surfaces is not well known.
Objectives: To compare and contrast ATV-related deaths on paved versus unpaved roads.
Methods: Retrospective descriptive and multivariable analyses were performed using Consumer Product Safety Commission fatality data from 1985-2009.
Results: Since 1998, the rate of increase in ATV-related deaths was twice as high for paved versus unpaved roads. Still, 43% of all deaths occurred on unpaved roads. States varied considerably ranging from only 16% up to 87% of their ATV-related deaths occurring on unpaved roads. Adolescents and younger adults had the highest proportion of deaths on paved roads. Only about a third of all roadway deaths involved a collision with another vehicle. Collisions with other vehicles were less likely on unpaved roads, and when occurring were more likely to involve a truck than those on paved surfaces. The ATV was more likely to be hit by the other vehicle on paved roads, with the opposite being true on those unpaved. Helmet use was lower, alcohol use was higher, and head injuries were more common in paved road crashes. However, head injuries were still over 60% for unpaved road fatalities. Helmets were associated with a lower proportion of head injuries among riders on both road types.
Conclusion: ATV use on both paved and unpaved roads are a significant risk factor for crash-related death. The majority of fatalities in many states involve unpaved roads. Safety warnings should reflect the increased risk associated with ATV use on public roadways regardless of surface type. Governing bodies should not pass ordinances increasing ATV roadway access.
34. Mechanisms and Contributing Factors of Side-by-Side Vehicle Crashes
Joshua Godding1, Gerene Denning2, Charles A. Jennissen2. 1University of Iowa Carver College of Medicine, Iowa City, IA; 2University of Iowa Department of Emergency Medicine, Iowa City, IA
Background: Side-by-sides (SxSs), which includes utility vehicles (UTVs) and recreational off-highway vehicles, are off-road vehicles that have become increasingly popular over the past few years. There are no reports in the literature specifically addressing the epidemiology of SxS crashes.
Objectives: To evaluate SxS crashes with respect to demographics, crash mechanisms, and associated risk factors.
Methods: A retrospective chart review and analysis was performed of patients with injuries related to SxS vehicles from 2008-2013 at the University of Iowa Hospital.
Results: Thirty-three patients were identified. Two-thirds were males. Over half (55%) were children <16 years of age, and three-quarters were ≤25 years old. Over four-fifths of the crashes occurred during daylight, and about one-third occurred on roadways. The crash mechanism was a rollover for two-thirds of the victims. One male patient was a pedestrian hit by a UTV; this patient was not included in subsequent data analysis calculations. Of those in the SxS at the time of the crash, 45% were subsequently struck and/or pinned by the vehicle. Victims whose primary crash mechanism was a rollover were significantly more likely to be struck and/or be pinned by the vehicle than those ejected or involved in a collision (p=0.02). There were nearly as many passenger victims (44%) as drivers (56%), and a trend showed children more likely to be passengers (p=0.09). Still, nearly 40% of the child victims were drivers of the vehicle. No victims were wearing a helmet. Four-fifths of the victims were unrestrained. All six of the patients whose primary mechanism of injury was ejection from the vehicle were children <16 years and unrestrained. Of these six ejections, four occurred on roadways. One-half of adult victims were obese with a BMI ≥30; none of the child victims were obese. Of adults tested for alcohol (70%), two-thirds were positive. All intoxicated patients were male and involved in rollovers, and five out of the six were obese or overweight.
Conclusion: Although most current SxS models have roll bars, lack of safety belt use is reducing their benefit. Youth suffer a high percentage of the injuries related to SxSs, often while driving. Children should be prohibited from operating SxSs. Certain adult populations appear at risk and may require targeted interventions.
35. Methodology Validation of Using Motion-Activated Cameras to Estimate Off-Highway Vehicle Park Census Data and Evaluate Rider Safety Behaviors
Emily Robinson1, Charles A. Jennissen1, Eilis Baranow1, Gabe Greene1, Kristel Wetjen2, Pam Hoogerwerf3, Gerene Denning1. 1University of Iowa Department of Emergency Medicine, Iowa City, IA; 2University of Iowa Division of Pediatric Surgery, Iowa City, IA; 3University of Iowa Children's Hospital, Iowa City, IA
Background: Safety behaviors of all-terrain vehicle (ATV) riders at off-highway vehicle (OHV) parks may be better than those riding off-road elsewhere. A previous study of trauma patients from Iowa OHV parks were significantly more likely to have been helmeted, and less likely to have been a passenger than those injured off-road outside of parks. Census data is required to determine if the significant differences found in the number of injured victims among OHV parks can be explained by higher use or if other factors are involved.
Objectives: To ascertain the photographic capture rate of riders entering OHV parks with motion-activated cameras, and to determine demographic, vehicle, and safety behavior variable concordance between on-site evaluations and photo appraisement for study validation purposes.
Methods: Panoramic motion-activated cameras were placed at the entrances of all eight public OHV parks in Iowa. Three investigators did on-site data collection and photo image analysis for demographic, vehicle, and safety behavior variables, with no investigator performing both the on-site and photo analysis for any particular camera. Data collected from on-site assessment was compared to that from photo evaluation.
Results: On-site data collection was performed for a total of 114 hours for 17 cameras during which a total of 493 off-road vehicles entered the OHV parks. A total of 251 vehicles were identified on photos for an overall capture rate by the motion-activated cameras of 50.9%. For cameras with at least 5 vehicles noted during on-site evaluation, the capture rate ranged from 38-81%. The number of vehicles entering the parks was segmented by 15 minute intervals and there was no significant variance or decrease in photo capture rate until there were more than 15 vehicles entering a park during a quarter hour period. Variable concordance between on-site and photo derived data ranged from 91-100% which included sex of rider, estimated age group of rider, vehicle type, number of wheels, number of riders on the vehicle, helmet use, and restraint use for side-by-side vehicles.
Conclusion: About one-half of riders entering Iowa OHV parks were able to be captured by motion-activated cameras. Our findings should allow park census estimation from photo-derived data. Concordance of study variables was high between that collected on-site and from photo assessment.
36. Off-Road Vehicle Regulation Enforcement at Iowa Off-Highway Vehicle Parks
Benjamin Wilkinson, Gerene Denning, Charles A. Jennissen. University of Iowa Department of Emergency Medicine, Iowa City, IA
Background: The number of off-highway vehicle (OHV) parks continues to grow to match the increasing popularity of off-road vehicles. Little is known about how park regulations and enforcement affect safety behavior among users. A previous study found that trauma patients from Iowa OHV parks were significantly more likely to be in compliance with all-terrain vehicle (ATV) safety regulations and behaviors than those injured off-road outside of parks . Although certain ATV regulations exist outside of OHV parks, their effects have been somewhat limited due to a lack of enforcement.
Objectives: To determine the types of enforcement performed by Department of Natural Resources (DNR) patrol officers in Iowa OHV parks and which regulations they enforce including the number of citations written for specific Iowa code violations.
Methods: Patrol officer time logs and enforcement activities were obtained through a cooperative agreement with the DNR. Enforcement activities (including verbal warnings, written warnings and written citations) and variables regarding to whom enforcement activities were directed were analyzed.
Results: During 455 hours of enforcement over 78 days, ATV patrol officers recorded 172 separate enforcement activities involving 166 individuals. Of these, 45% were verbal warnings, 51% were written warnings, and 4% were written citations. About 87% of enforcement activities were directed at males; there was a trend for females to more likely receive verbal warnings versus written warnings/citations when compared to males (p=0.08). A trend was also seen for those ≥40 years old to more likely receive verbal warnings as compared to younger adults (p=0.055). Individuals 16 to <30 years received the majority of enforcement (50%). Safety violations were the majority of infractions (53.5%). However, violations related to registration and ID display were significantly more likely to receive a written warning/citation compared to those related to safety behavior (p<0.0001).
Conclusion: Enforcement by patrol officers in Iowa OHV parks is primarily through warnings, and violators are allowed to correct their regulatory deficiencies; few written citations are administered. Further study will be needed to determine if safety behavior compliance is better during times when patrol officers are performing on-site enforcement as compared to when they are absent.
Charles A. Jennissen1, Joshua Godding2, Karisa Harland1, Gerene Denning1. 1University of Iowa Department of Emergency Medicine, Iowa City, IA; 2University of Iowa Carver College of Medicine, Iowa City, IA
Background: Traditional all-terrain vehicles (ATVs) are designed for one rider only. ATVs require “active riding,” meaning that the operator needs to assess changes in stability and rapidly adjust body position to compensate. Passengers likely alter the ability for drivers to actively ride and increase the center of gravity. Although passengers on ATVs are a known risk factor, how they contribute to crash likelihood and injury severity has not been well described.
Objectives: To better understand the effect passengers have on the mechanisms and injuries seen in ATV crashes.
Methods: A retrospective chart review and analysis was performed of ATV-related injuries from 2002-2013 at University of Iowa Hospitals.
Results: 538 cases were identified of which 20% were passengers or drivers with passengers. Both children and females were more likely to be passengers (p<0.0001). Although helmet use was low (~20%), drivers were more likely to wear helmets than passengers (p<0.01). Rollovers (49%) were the most common mechanism of injury. The victim was struck by their ATV in 19% and pinned in 10%. There was a trend seen that rollovers were more likely on sloped terrains with passengers. Backward rollovers were almost twice as likely to have passengers as all other rollovers and were also more likely to have passengers than non-rollovers. Victims who fell or were ejected to the rear were over seven times more likely to have been on an ATV with passengers than victims of other types of ejection (p<0.01) or those not ejected (p<0.01), and also had worse head injuries. Self-ejections and forward ejections appeared less likely if passengers were present. Patients who self-ejected had the highest extremity injury scores but less severe head injuries than other falls and ejections.
Conclusion: Passengers on ATVs may be at greater risk for fall/ejection to the rear which appears to increase the risk of head injury. ATV operators who self-eject receive extremity injuries but may be more able to protect their heads; passengers limit the ability of a driver to self-eject when losing vehicle control. A strict no rider rule could reduce risk of some ATV crashes.
33. All-Terrain Vehicle-Related Fatalities: All Roads Lead to Tragedy
Gerene Denning, Karisa Harland, Charles A. Jennissen. University of Iowa Department of Emergency Medicine, Iowa City, IA
Background: All-terrain vehicles (ATVs) are for off-highway use only, and many of their features create increased risk with roadway travel. They have deep-treaded tires designed to grab, rather than grip-and-release the road. Most have a locked rear differential or fixed rear axle, which means the back wheels do not turn at a different rate when going around a curve. Thus, ATVs require a relatively wider turning radius. ATVs also have lower pressure tires, a high center of gravity and a narrow track, all of which increase the risk of loss of control on roadways. Although the vast majority of ATV use is off-road, over 60% of ATV-related fatalities occur on roadways. Despite this, the epidemiology of ATV-related deaths on different road surfaces is not well known.
Objectives: To compare and contrast ATV-related deaths on paved versus unpaved roads.
Methods: Retrospective descriptive and multivariable analyses were performed using Consumer Product Safety Commission fatality data from 1985-2009.
Results: Since 1998, the rate of increase in ATV-related deaths was twice as high for paved versus unpaved roads. Still, 43% of all deaths occurred on unpaved roads. States varied considerably ranging from only 16% up to 87% of their ATV-related deaths occurring on unpaved roads. Adolescents and younger adults had the highest proportion of deaths on paved roads. Only about a third of all roadway deaths involved a collision with another vehicle. Collisions with other vehicles were less likely on unpaved roads, and when occurring were more likely to involve a truck than those on paved surfaces. The ATV was more likely to be hit by the other vehicle on paved roads, with the opposite being true on those unpaved. Helmet use was lower, alcohol use was higher, and head injuries were more common in paved road crashes. However, head injuries were still over 60% for unpaved road fatalities. Helmets were associated with a lower proportion of head injuries among riders on both road types.
Conclusion: ATV use on both paved and unpaved roads are a significant risk factor for crash-related death. The majority of fatalities in many states involve unpaved roads. Safety warnings should reflect the increased risk associated with ATV use on public roadways regardless of surface type. Governing bodies should not pass ordinances increasing ATV roadway access.
34. Mechanisms and Contributing Factors of Side-by-Side Vehicle Crashes
Joshua Godding1, Gerene Denning2, Charles A. Jennissen2. 1University of Iowa Carver College of Medicine, Iowa City, IA; 2University of Iowa Department of Emergency Medicine, Iowa City, IA
Background: Side-by-sides (SxSs), which includes utility vehicles (UTVs) and recreational off-highway vehicles, are off-road vehicles that have become increasingly popular over the past few years. There are no reports in the literature specifically addressing the epidemiology of SxS crashes.
Objectives: To evaluate SxS crashes with respect to demographics, crash mechanisms, and associated risk factors.
Methods: A retrospective chart review and analysis was performed of patients with injuries related to SxS vehicles from 2008-2013 at the University of Iowa Hospital.
Results: Thirty-three patients were identified. Two-thirds were males. Over half (55%) were children <16 years of age, and three-quarters were ≤25 years old. Over four-fifths of the crashes occurred during daylight, and about one-third occurred on roadways. The crash mechanism was a rollover for two-thirds of the victims. One male patient was a pedestrian hit by a UTV; this patient was not included in subsequent data analysis calculations. Of those in the SxS at the time of the crash, 45% were subsequently struck and/or pinned by the vehicle. Victims whose primary crash mechanism was a rollover were significantly more likely to be struck and/or be pinned by the vehicle than those ejected or involved in a collision (p=0.02). There were nearly as many passenger victims (44%) as drivers (56%), and a trend showed children more likely to be passengers (p=0.09). Still, nearly 40% of the child victims were drivers of the vehicle. No victims were wearing a helmet. Four-fifths of the victims were unrestrained. All six of the patients whose primary mechanism of injury was ejection from the vehicle were children <16 years and unrestrained. Of these six ejections, four occurred on roadways. One-half of adult victims were obese with a BMI ≥30; none of the child victims were obese. Of adults tested for alcohol (70%), two-thirds were positive. All intoxicated patients were male and involved in rollovers, and five out of the six were obese or overweight.
Conclusion: Although most current SxS models have roll bars, lack of safety belt use is reducing their benefit. Youth suffer a high percentage of the injuries related to SxSs, often while driving. Children should be prohibited from operating SxSs. Certain adult populations appear at risk and may require targeted interventions.
35. Methodology Validation of Using Motion-Activated Cameras to Estimate Off-Highway Vehicle Park Census Data and Evaluate Rider Safety Behaviors
Emily Robinson1, Charles A. Jennissen1, Eilis Baranow1, Gabe Greene1, Kristel Wetjen2, Pam Hoogerwerf3, Gerene Denning1. 1University of Iowa Department of Emergency Medicine, Iowa City, IA; 2University of Iowa Division of Pediatric Surgery, Iowa City, IA; 3University of Iowa Children's Hospital, Iowa City, IA
Background: Safety behaviors of all-terrain vehicle (ATV) riders at off-highway vehicle (OHV) parks may be better than those riding off-road elsewhere. A previous study of trauma patients from Iowa OHV parks were significantly more likely to have been helmeted, and less likely to have been a passenger than those injured off-road outside of parks. Census data is required to determine if the significant differences found in the number of injured victims among OHV parks can be explained by higher use or if other factors are involved.
Objectives: To ascertain the photographic capture rate of riders entering OHV parks with motion-activated cameras, and to determine demographic, vehicle, and safety behavior variable concordance between on-site evaluations and photo appraisement for study validation purposes.
Methods: Panoramic motion-activated cameras were placed at the entrances of all eight public OHV parks in Iowa. Three investigators did on-site data collection and photo image analysis for demographic, vehicle, and safety behavior variables, with no investigator performing both the on-site and photo analysis for any particular camera. Data collected from on-site assessment was compared to that from photo evaluation.
Results: On-site data collection was performed for a total of 114 hours for 17 cameras during which a total of 493 off-road vehicles entered the OHV parks. A total of 251 vehicles were identified on photos for an overall capture rate by the motion-activated cameras of 50.9%. For cameras with at least 5 vehicles noted during on-site evaluation, the capture rate ranged from 38-81%. The number of vehicles entering the parks was segmented by 15 minute intervals and there was no significant variance or decrease in photo capture rate until there were more than 15 vehicles entering a park during a quarter hour period. Variable concordance between on-site and photo derived data ranged from 91-100% which included sex of rider, estimated age group of rider, vehicle type, number of wheels, number of riders on the vehicle, helmet use, and restraint use for side-by-side vehicles.
Conclusion: About one-half of riders entering Iowa OHV parks were able to be captured by motion-activated cameras. Our findings should allow park census estimation from photo-derived data. Concordance of study variables was high between that collected on-site and from photo assessment.
36. Off-Road Vehicle Regulation Enforcement at Iowa Off-Highway Vehicle Parks
Benjamin Wilkinson, Gerene Denning, Charles A. Jennissen. University of Iowa Department of Emergency Medicine, Iowa City, IA
Background: The number of off-highway vehicle (OHV) parks continues to grow to match the increasing popularity of off-road vehicles. Little is known about how park regulations and enforcement affect safety behavior among users. A previous study found that trauma patients from Iowa OHV parks were significantly more likely to be in compliance with all-terrain vehicle (ATV) safety regulations and behaviors than those injured off-road outside of parks . Although certain ATV regulations exist outside of OHV parks, their effects have been somewhat limited due to a lack of enforcement.
Objectives: To determine the types of enforcement performed by Department of Natural Resources (DNR) patrol officers in Iowa OHV parks and which regulations they enforce including the number of citations written for specific Iowa code violations.
Methods: Patrol officer time logs and enforcement activities were obtained through a cooperative agreement with the DNR. Enforcement activities (including verbal warnings, written warnings and written citations) and variables regarding to whom enforcement activities were directed were analyzed.
Results: During 455 hours of enforcement over 78 days, ATV patrol officers recorded 172 separate enforcement activities involving 166 individuals. Of these, 45% were verbal warnings, 51% were written warnings, and 4% were written citations. About 87% of enforcement activities were directed at males; there was a trend for females to more likely receive verbal warnings versus written warnings/citations when compared to males (p=0.08). A trend was also seen for those ≥40 years old to more likely receive verbal warnings as compared to younger adults (p=0.055). Individuals 16 to <30 years received the majority of enforcement (50%). Safety violations were the majority of infractions (53.5%). However, violations related to registration and ID display were significantly more likely to receive a written warning/citation compared to those related to safety behavior (p<0.0001).
Conclusion: Enforcement by patrol officers in Iowa OHV parks is primarily through warnings, and violators are allowed to correct their regulatory deficiencies; few written citations are administered. Further study will be needed to determine if safety behavior compliance is better during times when patrol officers are performing on-site enforcement as compared to when they are absent.